You might also like
- Manage HypoglycemiaDocument57 pagesManage HypoglycemiaAmelia PricopNo ratings yet
- Pituitary Tumors Engleza 2Document89 pagesPituitary Tumors Engleza 2Achmad Harun MuchsinNo ratings yet
- Presentation On Hepatic Failure: Presented By: Sandhya Harbola M.SC Nursing 1 Year PcnmsDocument54 pagesPresentation On Hepatic Failure: Presented By: Sandhya Harbola M.SC Nursing 1 Year PcnmsShubham Singh BishtNo ratings yet
- Antidepressants: I. Cyclic AntidepressantDocument17 pagesAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaNo ratings yet
- Drug Compliance Among Hypertensive PatientsDocument5 pagesDrug Compliance Among Hypertensive PatientsSyifa MunawarahNo ratings yet
- Case Study 2Document37 pagesCase Study 2api-391842100No ratings yet
- Hormones of The Adrenal Cortex 1-13Document47 pagesHormones of The Adrenal Cortex 1-13abstabs50% (2)
- Nephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HDocument60 pagesNephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HJaiganesh MuruganandamNo ratings yet
- Esophageal CancerDocument25 pagesEsophageal CancerK poojithaNo ratings yet
- Medscape Status EpilepticusDocument10 pagesMedscape Status EpilepticusEllen Siska SusantiNo ratings yet
- Insulin and Oral Hypoglycemic DrugsDocument30 pagesInsulin and Oral Hypoglycemic DrugsAngga NugrahaNo ratings yet
- Approach To Septic ShockDocument16 pagesApproach To Septic ShockRaja EllysyaNo ratings yet
- Lung Cancer Types & TreatmentsDocument45 pagesLung Cancer Types & TreatmentsHowell Thomas Montilla AlamoNo ratings yet
- Sepsis Power Point Slide Presentation - The Guidelines - Implementation For The FutureDocument25 pagesSepsis Power Point Slide Presentation - The Guidelines - Implementation For The Futuremontie13No ratings yet
- (Pelvic Inflammatory Disease) Samiya AhmedDocument31 pages(Pelvic Inflammatory Disease) Samiya AhmedSaamiya AhmedNo ratings yet
- Management of Lymphomas: 2018 Indian Expert ConsensusDocument24 pagesManagement of Lymphomas: 2018 Indian Expert ConsensusAndi SusiloNo ratings yet
- Presentation SWINE FLUDocument40 pagesPresentation SWINE FLUdr_hammadNo ratings yet
- Adrenal Hormone 2018 PDFDocument66 pagesAdrenal Hormone 2018 PDFrosyidafiaNo ratings yet
- Systemic Lupus Erythematosus (SLE)Document39 pagesSystemic Lupus Erythematosus (SLE)Nadya SabrinaNo ratings yet
- Idiopathic Pulmonary Fibrosis: Optimizing The Diagnosis and Multi-Disciplinary Decision MakingDocument4 pagesIdiopathic Pulmonary Fibrosis: Optimizing The Diagnosis and Multi-Disciplinary Decision MakingAnna LiachenkoNo ratings yet
- Manual 24 Hour RecallDocument160 pagesManual 24 Hour RecallMadalina CervidNo ratings yet
- Fulminant Hepatic Failure: Nattaphol UransilpDocument27 pagesFulminant Hepatic Failure: Nattaphol UransilpChacha TasyaNo ratings yet
- Kidney TransplantDocument11 pagesKidney TransplantPrincess Xzmae RamirezNo ratings yet
- Nephrotic SyndromeeDocument28 pagesNephrotic SyndromeeRiteka SinghNo ratings yet
- Clinicians Handbook of DiabetesDocument227 pagesClinicians Handbook of DiabetesAndra PetroiuNo ratings yet
- Fluid Management - Presentation PDFDocument16 pagesFluid Management - Presentation PDFjuniorebinda100% (1)
- Ectopic PregnancyDocument76 pagesEctopic PregnancyVivian Jean TapayaNo ratings yet
- Liver Cirrhosis PowerPointDocument12 pagesLiver Cirrhosis PowerPointFrancis Adrian100% (2)
- Diabetes MellitusDocument8 pagesDiabetes MellitusJaja RamosNo ratings yet
- Acute Kidney InjuryDocument21 pagesAcute Kidney InjuryAtif Gazali100% (1)
- Type 2 Diabetes Mellitus - A Review of Current TrendsDocument5 pagesType 2 Diabetes Mellitus - A Review of Current TrendsRevivo RindaNo ratings yet
- Hepatic EncephalopathyDocument11 pagesHepatic Encephalopathyjulius billiNo ratings yet
- Reiki Therapy Reduces HypertensionDocument34 pagesReiki Therapy Reduces HypertensionYayu AlawiiahNo ratings yet
- MeningitisDocument12 pagesMeningitisFaith Vaughn100% (2)
- Glomerulonephritis: Nameesha Natasha Naidu 20130105Document26 pagesGlomerulonephritis: Nameesha Natasha Naidu 20130105AliMalikNo ratings yet
- HypothyroidismDocument54 pagesHypothyroidismagakshat23No ratings yet
- Thalassemias and HemoglobinopathiesDocument63 pagesThalassemias and HemoglobinopathiesMahmod_Al_Bust_4830No ratings yet
- HIV Disease and NutritionDocument10 pagesHIV Disease and Nutritionmariosan81No ratings yet
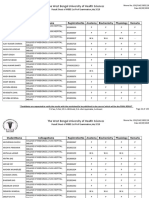
- The West Bengal University of Health SciencesDocument9 pagesThe West Bengal University of Health Sciencesbhaskar rayNo ratings yet
- Rapid Response Team Whitepaper With Intro UPDATEDDocument24 pagesRapid Response Team Whitepaper With Intro UPDATEDHari Mas KuncoroNo ratings yet
- Disseminated Intravascular CoagulationDocument2 pagesDisseminated Intravascular CoagulationVince100% (1)
- Drugs Effecting On Thyroid Gland: Abdullaev Dzhumadil, PharmdDocument22 pagesDrugs Effecting On Thyroid Gland: Abdullaev Dzhumadil, PharmdRtxGaming Zone 73No ratings yet
- Cirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDocument21 pagesCirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDan ChicinasNo ratings yet
- Congestive Cardiac Failure by NeetaDocument26 pagesCongestive Cardiac Failure by NeetaNeeta AnandaNo ratings yet
- DiabeticcasestudyDocument7 pagesDiabeticcasestudyapi-272773859No ratings yet
- Grave'S Disease: Farida Ulfa 1510211057Document11 pagesGrave'S Disease: Farida Ulfa 1510211057farida ulfaNo ratings yet
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocument4 pagesRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniNo ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeJawad SaleemNo ratings yet
- Brain TumorDocument50 pagesBrain TumorbudiNo ratings yet
- Congestive Cardiac FailureDocument20 pagesCongestive Cardiac FailureAnand VaghasiyaNo ratings yet
- Hemodiafiltration Kuhlmann PDFDocument31 pagesHemodiafiltration Kuhlmann PDFDavid SantosoNo ratings yet
- 1 Early Management of Trauma Patient in The HospitalDocument23 pages1 Early Management of Trauma Patient in The HospitalkgnmatinNo ratings yet
- Hypertension: Mayur BV BPH 3 Semester PSPHDocument29 pagesHypertension: Mayur BV BPH 3 Semester PSPHBijay Kumar MahatoNo ratings yet
- Hepatitis GDocument8 pagesHepatitis Ghelmi0% (1)
- LeprosyDocument16 pagesLeprosyNipul MondolNo ratings yet
- Hyporeninemic HypoaldosteronismDocument12 pagesHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisNo ratings yet
- Fulminant Hepatic FailureDocument12 pagesFulminant Hepatic Failureafghansyah arfiantoNo ratings yet
- Classifications of Thyroid TumoursDocument15 pagesClassifications of Thyroid TumoursSandra LisaNo ratings yet
- Practical Gastroenterology and Hepatology Board Review ToolkitFrom EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultNo ratings yet
- Election Commission of India Model Code of Conduct (2019)Document312 pagesElection Commission of India Model Code of Conduct (2019)Deepak Kumar VasudevanNo ratings yet
- QB Cardoiology 2015Document49 pagesQB Cardoiology 2015Amirsalar EslamiNo ratings yet
- Increase Cpu Speed Settings PDFDocument1 pageIncrease Cpu Speed Settings PDFRitesh SinghNo ratings yet
- 2013-14 Sports Medicine Handbook PDFDocument140 pages2013-14 Sports Medicine Handbook PDFVladimirNo ratings yet
- Lymphatic Filariasis Diagnosis & ManagementDocument3 pagesLymphatic Filariasis Diagnosis & ManagementRitesh SinghNo ratings yet
- Ecg Graphs ExplainedDocument147 pagesEcg Graphs ExplainedRitesh SinghNo ratings yet
- Cancer Caused by Fast Food ChemicalsDocument7 pagesCancer Caused by Fast Food ChemicalsRitesh SinghNo ratings yet
- Orthopedics McqsDocument6 pagesOrthopedics McqsRitesh Singh0% (1)
- GENERAL KNOWLEDGE MCQsDocument22 pagesGENERAL KNOWLEDGE MCQsRitesh SinghNo ratings yet
- Clinical Significance of Laboratory Test ValuesDocument29 pagesClinical Significance of Laboratory Test ValuesRitesh Singh100% (6)
- Sciatica ExercisesDocument8 pagesSciatica ExercisesRitesh Singh100% (1)
- Alcoholic HepatitisDocument7 pagesAlcoholic HepatitisRitesh SinghNo ratings yet
- Medical PG NotesDocument27 pagesMedical PG NotesRitesh Singh50% (2)
- Drug of Choice in Various DiseasesDocument5 pagesDrug of Choice in Various DiseasesRitesh Singh100% (5)
- 3 Cardiology HemodynamicsDocument90 pages3 Cardiology HemodynamicsPravallika ReddyNo ratings yet
- Cross MatchingDocument5 pagesCross MatchingMustafa KhandgawiNo ratings yet
- Incontinence Case StudyDocument26 pagesIncontinence Case StudyRose AnnNo ratings yet
- Hearing Aid Parts and Types of Hearing LossDocument8 pagesHearing Aid Parts and Types of Hearing LossHugh JacobsNo ratings yet
- Acute Care PDFDocument509 pagesAcute Care PDFamatory1702No ratings yet
- MiliariaDocument10 pagesMiliarianovi rista anandaNo ratings yet
- Colonoscopy prep tips for people with a stomaDocument1 pageColonoscopy prep tips for people with a stomaMobeen RazaNo ratings yet
- Final Exam Flashcards - Easy NotecardsDocument41 pagesFinal Exam Flashcards - Easy NotecardsTalo MjNo ratings yet
- DR Robert Schneider HandoutDocument20 pagesDR Robert Schneider HandoutmirfanulhaqNo ratings yet
- Asuhan Pasien Dengan Terminall IllnessDocument50 pagesAsuhan Pasien Dengan Terminall IllnessCieciel Silviaa FebrianiiNo ratings yet
- Thyroid Disease in PregnancyDocument67 pagesThyroid Disease in PregnancySiti Fatimah100% (2)
- LVAD in An Hbo2 ChamberDocument5 pagesLVAD in An Hbo2 ChamberTony LeeNo ratings yet
- Detrol (Tolterodine)Document1 pageDetrol (Tolterodine)ENo ratings yet
- Nivedita Nimesh C VDocument2 pagesNivedita Nimesh C Vapi-278464951No ratings yet
- Neurology for the Non-Neurologist: Non-Parkinson's TremorsDocument23 pagesNeurology for the Non-Neurologist: Non-Parkinson's TremorsElizabeth Virginia100% (1)
- Florence NightingaleDocument3 pagesFlorence NightingaleAndreeaNo ratings yet
- C.C.D 6137 Gladys Anne Cristine P. AquinoDocument6 pagesC.C.D 6137 Gladys Anne Cristine P. Aquinoroneldayo62No ratings yet
- Emergency Trauma Flow SheetDocument4 pagesEmergency Trauma Flow SheetLili BritoNo ratings yet
- Placenta Previa NCP 1Document6 pagesPlacenta Previa NCP 1Faye Nervanna Alecha Alferez83% (18)
- About AyurvedaDocument10 pagesAbout AyurvedaUrvi SoniNo ratings yet
- A Prescription For Love by Tufano 79Document610 pagesA Prescription For Love by Tufano 79Victoria HernanNo ratings yet
- GastritisDocument206 pagesGastritisFaye Viray100% (2)
- Legal and Ethical Issues in Safe Blood TransfusionDocument7 pagesLegal and Ethical Issues in Safe Blood TransfusionaksinuNo ratings yet
- Lead PoisoningDocument17 pagesLead PoisoningParvez X GulNo ratings yet
- Oncologic NursingDocument16 pagesOncologic NursingDharline Abbygale Garvida AgullanaNo ratings yet
- Target Gene for "Pretzel SyndromeDocument6 pagesTarget Gene for "Pretzel Syndromesavvy_as_98-1No ratings yet
- Atrial Septal DefectDocument3 pagesAtrial Septal Defectsyahid_unsriNo ratings yet
- Dental Decks Periodontics DR GhadeerDocument162 pagesDental Decks Periodontics DR GhadeerGhadeerHassaan100% (11)
- ActonelDocument42 pagesActonelSimon JonatanNo ratings yet
- TungStyleOrthodox PDFDocument5 pagesTungStyleOrthodox PDFSifu LiceNo ratings yet