You might also like
- Organic NMR Spectroscopy ExplainedDocument57 pagesOrganic NMR Spectroscopy ExplainedAthina MardhaNo ratings yet
- Structural Analysis of FlavonoidsDocument25 pagesStructural Analysis of FlavonoidsAthina MardhaNo ratings yet
- Solid Phase Extraction - Macherel NargelDocument14 pagesSolid Phase Extraction - Macherel NargelAthina MardhaNo ratings yet
- Mass Spec LectureDocument52 pagesMass Spec LectureAthina MardhaNo ratings yet
- EMA - Guideline On Bioanalytical Method ValidationDocument22 pagesEMA - Guideline On Bioanalytical Method ValidationprenatooliveiraNo ratings yet
- Who HerbalDocument82 pagesWho HerbalgauthamankNo ratings yet
- Hvac PDFDocument172 pagesHvac PDFAthina Mardha67% (3)
- Amerchol L101Document1 pageAmerchol L101Athina MardhaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Form G - Disability Verification - 5-18-2021 - EnglishDocument3 pagesForm G - Disability Verification - 5-18-2021 - EnglishtavoNo ratings yet
- Hydrochloric Acid MSDS: 1. Product and Company IdentificationDocument7 pagesHydrochloric Acid MSDS: 1. Product and Company IdentificationdeaNo ratings yet
- PresentationDocument8 pagesPresentationShubhamNo ratings yet
- Care Plan Presentation On Meningitis PatientDocument20 pagesCare Plan Presentation On Meningitis PatientDuop Jock LiemNo ratings yet
- Ace Personal Trainer Chapter 3Document45 pagesAce Personal Trainer Chapter 3Daan van der Meulen100% (2)
- Q and A Legal MedicineDocument10 pagesQ and A Legal MedicineQayes Al-QuqaNo ratings yet
- AlluloseDocument2 pagesAlluloseJagadeesh KumarNo ratings yet
- 4 FFBDocument7 pages4 FFBDian Ika CahyaniNo ratings yet
- What Is Aquatic TherapyDocument5 pagesWhat Is Aquatic TherapyHaslindaNo ratings yet
- Case Study On Acute GlomerulonephritisDocument20 pagesCase Study On Acute GlomerulonephritisJai - Ho87% (15)
- EM Basic Chest Pain: Pet Mac P E T M A CDocument7 pagesEM Basic Chest Pain: Pet Mac P E T M A CAkanksha VermaNo ratings yet
- Hope Ziua 3Document2 pagesHope Ziua 3Ancuta Si Ionut CazamirNo ratings yet
- Prescriptions And: Medication OrdersDocument67 pagesPrescriptions And: Medication OrdersGraizel Joy Andres100% (1)
- Suggestive Questions of Isc 2023 BiologyDocument12 pagesSuggestive Questions of Isc 2023 Biologyjahnvipatel2004No ratings yet
- Law Update R.A. 10354Document2 pagesLaw Update R.A. 10354Jon MerazNo ratings yet
- Micronutrient Deficiencies ExplainedDocument34 pagesMicronutrient Deficiencies ExplainedRegita Trimulia100% (1)
- Student X IepDocument6 pagesStudent X Iepapi-566781582No ratings yet
- Chronic Respiratory Disease in Poultry Case ReportDocument5 pagesChronic Respiratory Disease in Poultry Case ReportPandu AWUNo ratings yet
- 55122505241#5852#55122505241#9 - 16 - 2022 12 - 00 - 00 AmDocument2 pages55122505241#5852#55122505241#9 - 16 - 2022 12 - 00 - 00 AmAdham ZidanNo ratings yet
- RadPRO Soltus 100M Mobile Digital X-Ray System Operator's Manual - ADocument124 pagesRadPRO Soltus 100M Mobile Digital X-Ray System Operator's Manual - AAdam Malzewski100% (3)
- Have You Ever Phoned For An ?: AmbulanceDocument2 pagesHave You Ever Phoned For An ?: AmbulanceAléxia AndradeNo ratings yet
- Thromboembolic Complications in Chronic Inflammatory Bowel DiseaseDocument6 pagesThromboembolic Complications in Chronic Inflammatory Bowel DiseaseIJAR JOURNALNo ratings yet
- Postpartum Hemorrhage: A.Personal DataDocument55 pagesPostpartum Hemorrhage: A.Personal DataEmmanuel Recodo100% (1)
- ch03 PDFDocument17 pagesch03 PDFJessica nonyeNo ratings yet
- tmp342C TMPDocument182 pagestmp342C TMPFrontiers100% (1)
- Datasheet of Imisopasem-Manganese (M40403) - CAS 218791-21-0Document2 pagesDatasheet of Imisopasem-Manganese (M40403) - CAS 218791-21-0LouisNo ratings yet
- Comparison On Efficiency of Various Techniques in Biological Treatment of Effluent Water - Final 2Document8 pagesComparison On Efficiency of Various Techniques in Biological Treatment of Effluent Water - Final 2desai sanketNo ratings yet
- Pqa Executive Fellow Q ADocument3 pagesPqa Executive Fellow Q Aapi-407904109No ratings yet
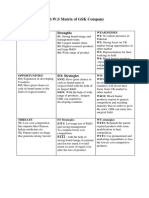
- Tows GSKDocument2 pagesTows GSKQanita Shah100% (2)
- HN Webinar Healthy Gut Healthy You November 2023Document39 pagesHN Webinar Healthy Gut Healthy You November 2023ramcm024No ratings yet