You might also like
- Kebijakan High AlertDocument8 pagesKebijakan High AlertheavyrainNo ratings yet
- Alcoholic CardiomyopathyDocument9 pagesAlcoholic CardiomyopathyheavyrainNo ratings yet
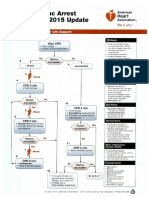
- ACLS 2015 Algorithm PDFDocument8 pagesACLS 2015 Algorithm PDFheavyrain100% (1)
- Benign Positional Vertigo: Taleb Mohammed Mansoor Khaleil Ebrahem Al-MatroushiDocument27 pagesBenign Positional Vertigo: Taleb Mohammed Mansoor Khaleil Ebrahem Al-MatroushiSheila CantikNo ratings yet
- Eye EmergenciesDocument18 pagesEye EmergenciesdrDre91No ratings yet
- Pathogenesis Liver InvolvementDocument7 pagesPathogenesis Liver InvolvementheavyrainNo ratings yet
- Acute Coronary SyndromeDocument19 pagesAcute Coronary SyndromeheavyrainNo ratings yet
- BPPVDocument27 pagesBPPVheavyrainNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- HuddersfieldDocument1 pageHuddersfieldNdumiso MoyoNo ratings yet
- International Undergraduate Prospectus 2015 2016Document130 pagesInternational Undergraduate Prospectus 2015 2016Juank GarcésNo ratings yet
- Outbreaks Epidemics and Pandemics ReadingDocument2 pagesOutbreaks Epidemics and Pandemics Readingapi-290100812No ratings yet
- Genital Herpes: Aarthi (2012)Document36 pagesGenital Herpes: Aarthi (2012)Aiman TymerNo ratings yet
- MyiasisDocument3 pagesMyiasisMohiedden M Abdul-FattahNo ratings yet
- Application Form Defacto SpecialistsDocument6 pagesApplication Form Defacto SpecialistsNancy De BriyneNo ratings yet
- NKC Fast Facts - Poop Chart - 5 2017 PDFDocument1 pageNKC Fast Facts - Poop Chart - 5 2017 PDFFaniaNo ratings yet
- BruvaxDocument1 pageBruvaxArif K BashaNo ratings yet
- Chain of InfectionDocument13 pagesChain of InfectionPrince Jhessie L. AbellaNo ratings yet
- Kode IcdDocument5 pagesKode IcdNurul FatimahNo ratings yet
- Mortalidad AnestesicaDocument10 pagesMortalidad AnestesicaPaula Andrea RodriguezNo ratings yet
- Mumps Guide: Causes, Symptoms, Treatment & PreventionDocument14 pagesMumps Guide: Causes, Symptoms, Treatment & PreventionChristian JonathanNo ratings yet
- Fungal Infections in Cattle in A Gaushala at Jaipur: Haryana Vet. 49 (December, 2010), PP 62-63Document2 pagesFungal Infections in Cattle in A Gaushala at Jaipur: Haryana Vet. 49 (December, 2010), PP 62-63Mahavir DamakaleNo ratings yet
- Appendix - 1: List of ICI Journal Titles Pending EvaluationDocument7 pagesAppendix - 1: List of ICI Journal Titles Pending EvaluationMultan Singh BhatiNo ratings yet
- 1040 A Day in The Life of A Veterinary Technician PDFDocument7 pages1040 A Day in The Life of A Veterinary Technician PDFSedat KorkmazNo ratings yet
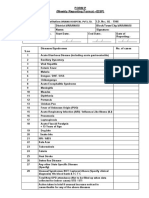
- Form P (Weekly Reporting Format - IDSP) : Oriana Hospital PVT - LTDDocument2 pagesForm P (Weekly Reporting Format - IDSP) : Oriana Hospital PVT - LTDRavi ParmarNo ratings yet
- What Is Mumps in ChildrenDocument4 pagesWhat Is Mumps in ChildrenFoster K KaundaNo ratings yet
- Alexis Wolter ResumeDocument2 pagesAlexis Wolter Resumeapi-610069547No ratings yet
- Droplet Infection: Tuberkulosis (TB) ParuDocument2 pagesDroplet Infection: Tuberkulosis (TB) ParuMiiniieNo ratings yet
- Basic TB FactsDocument8 pagesBasic TB FactshatemfaroukNo ratings yet
- Pathogenic Variants Persistent Infections Emerging Viruses Antigenic Variation Zoonotic DiseaseDocument28 pagesPathogenic Variants Persistent Infections Emerging Viruses Antigenic Variation Zoonotic DiseaseSantosh BhandariNo ratings yet
- Company Profile Ayulia 2023Document13 pagesCompany Profile Ayulia 2023Willia HospitalNo ratings yet
- Epi ReviewerDocument4 pagesEpi ReviewerHannah VueltaNo ratings yet
- Iceberg DiseasesDocument18 pagesIceberg Diseasesachuth29No ratings yet
- Recapitulare TestDocument38 pagesRecapitulare TestDana ChitoiNo ratings yet
- Laboratory Report: Name: MR .Sandeep Mane Patient ID: P80359Document1 pageLaboratory Report: Name: MR .Sandeep Mane Patient ID: P80359akash srivastavaNo ratings yet
- Dengue Fever: Centre For Health Protection, Department of Health July 2019Document17 pagesDengue Fever: Centre For Health Protection, Department of Health July 2019Melissa Marie CustodioNo ratings yet
- Backyard Poultry Medicine and Surgery - A Guide For Veterinary Practitioners, 2nd EditionDocument672 pagesBackyard Poultry Medicine and Surgery - A Guide For Veterinary Practitioners, 2nd EditionAbubakar Tahir Ramay100% (1)
- Chickenpox (Varicella) : A Communicable DiseaseDocument12 pagesChickenpox (Varicella) : A Communicable DiseaseEizel Nhey G. JADENo ratings yet
- Virology Learning TableDocument6 pagesVirology Learning Table//No ratings yet