You might also like
- Pemeriksaan Hasil Nilai Normal Puasa: 80-120: Gula Darah Sewaktu 140Document1 pagePemeriksaan Hasil Nilai Normal Puasa: 80-120: Gula Darah Sewaktu 140Fatt ZakiNo ratings yet
- Septal PerforationDocument23 pagesSeptal PerforationFatt ZakiNo ratings yet
- H 100696Document26 pagesH 100696Fatt ZakiNo ratings yet
- Complicated Urinary Tract Infection in Adults: Ammi Guideline PaperDocument22 pagesComplicated Urinary Tract Infection in Adults: Ammi Guideline PaperFatt ZakiNo ratings yet
- Airway ManagementDocument31 pagesAirway Managementiqiqiqiqiq100% (1)
- Aimed Competency:: Rendering Quality Care Through Disciplined Medical CareDocument32 pagesAimed Competency:: Rendering Quality Care Through Disciplined Medical CareFatt ZakiNo ratings yet
- Tionnairejobsatisfaction Compensation ProductivityDocument5 pagesTionnairejobsatisfaction Compensation ProductivityFatt ZakiNo ratings yet
- DcjsdaDocument13 pagesDcjsdaFatt ZakiNo ratings yet
- What Is Brucellosis?Document6 pagesWhat Is Brucellosis?Fatt ZakiNo ratings yet
- Modul 7 CPCRDocument2 pagesModul 7 CPCRFatt ZakiNo ratings yet
- Modul 2 Intravenous CatheterDocument1 pageModul 2 Intravenous CatheterBirgitta FajaraiNo ratings yet
- Kuliah Obgyn EmergencyDocument37 pagesKuliah Obgyn EmergencyFatt ZakiNo ratings yet
- Management BetaDocument1 pageManagement Betarahman_alfarisiNo ratings yet
- Digital Booklet - WhiplashDocument7 pagesDigital Booklet - WhiplashArnie50% (2)
- Emergency Obs NStranslatedDocument45 pagesEmergency Obs NStranslatedFatt ZakiNo ratings yet
- Psychiatric EmergenciesDocument23 pagesPsychiatric EmergenciesFatt ZakiNo ratings yet
- Psychiatric EmergenciesDocument23 pagesPsychiatric EmergenciesFatt ZakiNo ratings yet
- Win32 file hashes and metadataDocument109 pagesWin32 file hashes and metadataCarlo CondeNo ratings yet
- Psychiatric EmergenciesDocument23 pagesPsychiatric EmergenciesFatt ZakiNo ratings yet
- Musculoskeletal Trauma GuideDocument99 pagesMusculoskeletal Trauma GuideFatt ZakiNo ratings yet
- TEAM For Medical StudentsDocument79 pagesTEAM For Medical StudentsFatt ZakiNo ratings yet
- RCTS Clinical Trials RandomizationDocument35 pagesRCTS Clinical Trials RandomizationFatt ZakiNo ratings yet
- Shock & Management ConceptDocument109 pagesShock & Management ConceptFatt ZakiNo ratings yet
- Developing Research Ideas Through Literature ReviewDocument36 pagesDeveloping Research Ideas Through Literature ReviewFatt ZakiNo ratings yet
- PHYLOSOPHYDocument32 pagesPHYLOSOPHYFatt ZakiNo ratings yet
- The Relationship Between Caffeine Consumption and OsteoporosisDocument15 pagesThe Relationship Between Caffeine Consumption and OsteoporosisFatt ZakiNo ratings yet
- Pain Management in DentistryDocument9 pagesPain Management in DentistryFatt ZakiNo ratings yet
- AKL I Ch06 Beams10e SMDocument39 pagesAKL I Ch06 Beams10e SMDwiApriliyaniNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chapter 3Document11 pagesChapter 3Leu Gim Habana PanuganNo ratings yet
- Supplier of PesticidesDocument2 pagesSupplier of PesticidestusharNo ratings yet
- The Hittite Name For GarlicDocument5 pagesThe Hittite Name For GarlictarnawtNo ratings yet
- Rev Transcription Style Guide v3.3Document18 pagesRev Transcription Style Guide v3.3jhjNo ratings yet
- Official Website of the Department of Homeland Security STEM OPT ExtensionDocument1 pageOfficial Website of the Department of Homeland Security STEM OPT ExtensionTanishq SankaNo ratings yet
- Christian Mission and Conversion. Glimpses About Conversion, Constitution, Right To ReligionDocument8 pagesChristian Mission and Conversion. Glimpses About Conversion, Constitution, Right To ReligionSudheer Siripurapu100% (1)
- 10 1108 - Apjie 02 2023 0027Document17 pages10 1108 - Apjie 02 2023 0027Aubin DiffoNo ratings yet
- Rock Art and Metal TradeDocument22 pagesRock Art and Metal TradeKavu RI100% (1)
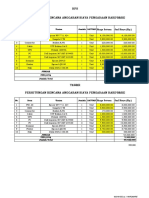
- HPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANDocument2 pagesHPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANYanto AstriNo ratings yet
- 1 Ancient-IndiaDocument14 pages1 Ancient-Indiakaushik joshiNo ratings yet
- Infinitive Clauses PDFDocument3 pagesInfinitive Clauses PDFKatia LeliakhNo ratings yet
- LS1 Eng. Modules With Worksheets (Figure of Speech)Document14 pagesLS1 Eng. Modules With Worksheets (Figure of Speech)Bong CardonaNo ratings yet
- CVA: Health Education PlanDocument4 pagesCVA: Health Education Plandanluki100% (3)
- Writing Assessment and Evaluation Checklist - PeerDocument1 pageWriting Assessment and Evaluation Checklist - PeerMarlyn Joy YaconNo ratings yet
- TDS Tetrapur 100 (12-05-2014) enDocument2 pagesTDS Tetrapur 100 (12-05-2014) enCosmin MușatNo ratings yet
- Unit 5 The Teacher As ProfessionalDocument23 pagesUnit 5 The Teacher As ProfessionalLeame Hoyumpa Mazo100% (5)
- Visual Basic 2019 Made Easy: by DR - LiewDocument33 pagesVisual Basic 2019 Made Easy: by DR - LiewAbhijit Jadhav100% (1)
- Diaz, Rony V. - at War's End An ElegyDocument6 pagesDiaz, Rony V. - at War's End An ElegyIan Rosales CasocotNo ratings yet
- A Chat (GPT) About The Future of Scientific PublishingDocument3 pagesA Chat (GPT) About The Future of Scientific Publishingraul kesumaNo ratings yet
- APP Eciation: Joven Deloma Btte - Fms B1 Sir. Decederio GaganteDocument5 pagesAPP Eciation: Joven Deloma Btte - Fms B1 Sir. Decederio GaganteJanjan ToscanoNo ratings yet
- Sky Education: Organisation of Commerce and ManagementDocument12 pagesSky Education: Organisation of Commerce and ManagementKiyaara RathoreNo ratings yet
- History of Downtown San Diego - TimelineDocument3 pagesHistory of Downtown San Diego - Timelineapi-671103457No ratings yet
- Comment On Motion To Release Vehicle BeridoDocument3 pagesComment On Motion To Release Vehicle BeridoRaffy PangilinanNo ratings yet
- LESSON 2 - Nguyễn Thu Hồng - 1917710050Document2 pagesLESSON 2 - Nguyễn Thu Hồng - 1917710050Thu Hồng NguyễnNo ratings yet
- TOPIC 12 Soaps and DetergentsDocument14 pagesTOPIC 12 Soaps and DetergentsKaynine Kiko50% (2)
- English FinalDocument321 pagesEnglish FinalManuel Campos GuimeraNo ratings yet
- FOREIGN DOLL CORP May 2023 TD StatementDocument4 pagesFOREIGN DOLL CORP May 2023 TD Statementlesly malebrancheNo ratings yet
- Republic vs. Maria Lee and IAC, G.R. No. 64818, May 13, 1991 (197 SCRA)Document1 pageRepublic vs. Maria Lee and IAC, G.R. No. 64818, May 13, 1991 (197 SCRA)PatNo ratings yet
- Training of Local Government Personnel PHDocument5 pagesTraining of Local Government Personnel PHThea ConsNo ratings yet
- Ck-Nac FsDocument2 pagesCk-Nac Fsadamalay wardiwiraNo ratings yet