You might also like
- Pediatric Omphalocele and Gastroschisis - Background, Pathophysiology, Epidemiology PDFDocument12 pagesPediatric Omphalocele and Gastroschisis - Background, Pathophysiology, Epidemiology PDFNena_mileyNo ratings yet
- Epidermal Skin BarrierDocument10 pagesEpidermal Skin BarrierNena_mileyNo ratings yet
- Pediatric Omphalocele and Gastroschisis - Background, Pathophysiology, Epidemiology PDFDocument12 pagesPediatric Omphalocele and Gastroschisis - Background, Pathophysiology, Epidemiology PDFNena_mileyNo ratings yet
- Pediatric Omphalocele and Gastroschisis - Background, Pathophysiology, EpidemiologyDocument12 pagesPediatric Omphalocele and Gastroschisis - Background, Pathophysiology, EpidemiologyNena_mileyNo ratings yet
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDocument1 pageJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandNo ratings yet
- Balance CairanDocument1 pageBalance CairanNena_mileyNo ratings yet
- Ttype 1 Diabetes in Adults Ype 1 Diabetes in Adults: About This Information About This InformationDocument21 pagesTtype 1 Diabetes in Adults Ype 1 Diabetes in Adults: About This Information About This InformationNena_mileyNo ratings yet
- OsteomalasiaDocument4 pagesOsteomalasiaNena_mileyNo ratings yet
- Weight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Document1 pageWeight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Malisa LukmanNo ratings yet
- Ventolin Respirator Solution: Product MonographDocument37 pagesVentolin Respirator Solution: Product MonographNena_mileyNo ratings yet
- 07.04.06 Non-Rebreathing MaskDocument3 pages07.04.06 Non-Rebreathing MaskNena_mileyNo ratings yet
- Denah Ruang IPDDocument1 pageDenah Ruang IPDNena_mileyNo ratings yet
- MalariaDocument7 pagesMalariaNena_miley100% (1)
- GINA SlideSet 2015Document170 pagesGINA SlideSet 2015Nena_mileyNo ratings yet
- 01 Editorial DyspepsiaDocument1 page01 Editorial DyspepsiaDiva Augusti DirgahayuNo ratings yet
- 018 W3310 12 PDFDocument51 pages018 W3310 12 PDFNena_mileyNo ratings yet
- CHT Lfa Girls Z 0 2Document1 pageCHT Lfa Girls Z 0 2Melly Selvia ANo ratings yet
- ATLS - AirwayDocument24 pagesATLS - AirwayNena_mileyNo ratings yet
- ANA TestDocument9 pagesANA TestNena_mileyNo ratings yet
- Blood Brain BarrierDocument6 pagesBlood Brain BarrierdamonsalvotoreNo ratings yet
- Diagnostic Test List For DehydrationDocument1 pageDiagnostic Test List For DehydrationNena_mileyNo ratings yet
- Diagnosa Banding Gangguan Somatisasi dan KonversiDocument3 pagesDiagnosa Banding Gangguan Somatisasi dan KonversiNena_mileyNo ratings yet
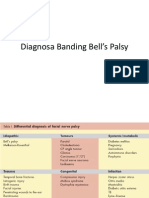
- Diagnosa Banding Bell's PalsyDocument5 pagesDiagnosa Banding Bell's PalsyNena_mileyNo ratings yet
- Kelompok Tutorial A1Document6 pagesKelompok Tutorial A1Nena_mileyNo ratings yet
- Diagnosa Banding Gangguan Somatisasi dan KonversiDocument3 pagesDiagnosa Banding Gangguan Somatisasi dan KonversiNena_mileyNo ratings yet
- Manifestasi Klinis AsmaDocument6 pagesManifestasi Klinis AsmaNena_mileyNo ratings yet
- DB15 - Asthma PharmacologyDocument3 pagesDB15 - Asthma PharmacologyNena_mileyNo ratings yet
- Manifestasi Klinis AsmaDocument6 pagesManifestasi Klinis AsmaNena_mileyNo ratings yet
- JakDocument68 pagesJakNena_mileyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nursing Care Analysis Record 2nd SemDocument29 pagesNursing Care Analysis Record 2nd SemDianneNo ratings yet
- Advanced Level Grammar Exercise MCQ Test 19Document4 pagesAdvanced Level Grammar Exercise MCQ Test 19Jerome Nayra ManansalaNo ratings yet
- University of University: Indigofera Zollingeriana R0: 0% R1: 4% R2: 8% R3: 12% and R4 16%Document7 pagesUniversity of University: Indigofera Zollingeriana R0: 0% R1: 4% R2: 8% R3: 12% and R4 16%Mas MeidiNo ratings yet
- Why Do We Sleep Thesis StatementDocument8 pagesWhy Do We Sleep Thesis Statementafcnenabv100% (2)
- Company Profile: How Aristagloves Became a Leader in Personal Protective EquipmentDocument16 pagesCompany Profile: How Aristagloves Became a Leader in Personal Protective EquipmentNissaaNo ratings yet
- Steps of Scientific Method: An IntroductionDocument13 pagesSteps of Scientific Method: An IntroductionAshiqur RahmanNo ratings yet
- Den 11Document167 pagesDen 11Marion HernandezNo ratings yet
- Dur 505 - 350Document9 pagesDur 505 - 350DebNo ratings yet
- XLD Series Vertical Stamper User ManualDocument78 pagesXLD Series Vertical Stamper User ManualGonzalo Marquez100% (1)
- Etiology of Liver Cirrhosis PDFDocument2 pagesEtiology of Liver Cirrhosis PDFAdamNo ratings yet
- Application, Usage, and Effectiveness of Testimony Therapy On Survivors of ViolenceDocument20 pagesApplication, Usage, and Effectiveness of Testimony Therapy On Survivors of Violencepvchr.india9214No ratings yet
- 13 Chapter 4Document31 pages13 Chapter 4HhuNo ratings yet
- Laboratory /workshop Inspection Checklist: Department of Chemical EngineeringDocument8 pagesLaboratory /workshop Inspection Checklist: Department of Chemical EngineeringAiman MuhammadNo ratings yet
- Nursing care plan for post-op cataract surgeryDocument2 pagesNursing care plan for post-op cataract surgeryFranz goNo ratings yet
- Statement of Purpose For Bachelor of Nursing CanadaDocument3 pagesStatement of Purpose For Bachelor of Nursing CanadachisomNo ratings yet
- DEMONSTRATION Antenatal EXERCISES DURING PREGNANCY PrintDocument10 pagesDEMONSTRATION Antenatal EXERCISES DURING PREGNANCY Printjyoti singh100% (1)
- DANC7782 Lab Report 10Document13 pagesDANC7782 Lab Report 10MaeNo ratings yet
- Test of Maslach Burnout Inventory Healthcare ProfessionalsDocument16 pagesTest of Maslach Burnout Inventory Healthcare ProfessionalsVagelis Karavelas100% (1)
- CONSENT TO PROCESS INFORMATION - Principal - Corporate RevDocument1 pageCONSENT TO PROCESS INFORMATION - Principal - Corporate RevAdonis Zoleta AranilloNo ratings yet
- Biodiversity and A Healthy Society: Group 2Document14 pagesBiodiversity and A Healthy Society: Group 2Dianna Lynn MolinaNo ratings yet
- NEET UG 2022 score card and rank for Parimi ManasaDocument1 pageNEET UG 2022 score card and rank for Parimi ManasaVidya SagarNo ratings yet
- Potential and impacts of nanotechnology on societyDocument4 pagesPotential and impacts of nanotechnology on societyAji Love SuropiaNo ratings yet
- Beisser - Paradoksalna Teorija PromeneDocument3 pagesBeisser - Paradoksalna Teorija PromeneBranka SuboticNo ratings yet
- IbandronatedrugscomDocument25 pagesIbandronatedrugscomroyNo ratings yet
- NLP and Hypnosis Reference BooksDocument9 pagesNLP and Hypnosis Reference BooksMarco Baratta100% (1)
- Type of Theories. CategoriesdocxDocument2 pagesType of Theories. CategoriesdocxMira Chariza Therese A. - BSN 1- CNo ratings yet
- Feras Mohammed Al Khayat: Core StrengthsDocument1 pageFeras Mohammed Al Khayat: Core StrengthsMona AlanaziNo ratings yet
- EOC Roles and ResponsibilitiesDocument8 pagesEOC Roles and ResponsibilitiesfowziNo ratings yet
- What Does The Phrase "Behavior Is Caused" Mean?: Montgomery, Jerald James G. Organizational BehaviorDocument10 pagesWhat Does The Phrase "Behavior Is Caused" Mean?: Montgomery, Jerald James G. Organizational Behaviorjerald james montgomeryNo ratings yet
- Experienced Healthcare AssistantDocument2 pagesExperienced Healthcare Assistantbroken bunny 191No ratings yet