You might also like
- Colorectal CancerDocument39 pagesColorectal CancerMuvenn Kannan100% (2)
- Orthopedics MCQs With AnswersDocument32 pagesOrthopedics MCQs With AnswerslanghalilafaNo ratings yet
- ACLS Pre-TestDocument24 pagesACLS Pre-TestBaltej Sidhu80% (10)
- NUR3111 Post-Lecture QuizDocument28 pagesNUR3111 Post-Lecture QuizliNo ratings yet
- Drugs used to treat cardiac arrhythmiasDocument74 pagesDrugs used to treat cardiac arrhythmiasGunel Sadiqova100% (1)
- Anaesthesia and Atrial FibrillationDocument15 pagesAnaesthesia and Atrial FibrillationNaresh Dhawan100% (1)
- EcgDocument18 pagesEcgDelyn Gamutan MillanNo ratings yet
- Cardiac Pacemakers NewDocument108 pagesCardiac Pacemakers NewAlif Fanharnita BrilianaNo ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
- Basics of Pacing CombinedDocument54 pagesBasics of Pacing CombinedMichael Susanto100% (1)
- Ecg Treadmill and Holter TestDocument77 pagesEcg Treadmill and Holter TestRiteka Singh100% (1)
- Assessment or Acute Renal Failure SymptomsDocument6 pagesAssessment or Acute Renal Failure SymptomsRifa Aprillia CahyaniNo ratings yet
- EkgDocument67 pagesEkgFendi Rafif Dad'sNo ratings yet
- ECG Flashcards: Atrial ArrhythmiasDocument27 pagesECG Flashcards: Atrial ArrhythmiasDima HabanjarNo ratings yet
- Focal Atrial Tachycardia I: Clinical Features, DiagnosisDocument10 pagesFocal Atrial Tachycardia I: Clinical Features, Diagnosisapi-26166949No ratings yet
- Implementation of Low Delay Dual Chamber Pacemaker Using VerilogDocument4 pagesImplementation of Low Delay Dual Chamber Pacemaker Using VerilogMeghanand KumarNo ratings yet
- Measure Intracardiac Pressures & Assess Cardiac FunctionDocument41 pagesMeasure Intracardiac Pressures & Assess Cardiac Functionwaleed315No ratings yet
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- Ecg 111029102429 Phpapp01Document103 pagesEcg 111029102429 Phpapp01Vickry WahidjiNo ratings yet
- ElectrocardiogramDocument52 pagesElectrocardiogramTuong HoangManhNo ratings yet
- Free Medical ECG Interpretation PresentationsDocument30 pagesFree Medical ECG Interpretation PresentationsRohini SelvarajahNo ratings yet
- Design and Analysis of A Dual Chamber Cardiac Pacemaker Using VHDL in Biomedical ApplicationDocument3 pagesDesign and Analysis of A Dual Chamber Cardiac Pacemaker Using VHDL in Biomedical ApplicationEditor IJRITCCNo ratings yet
- DefibrillationDocument9 pagesDefibrillationJara Maris Moreno BudionganNo ratings yet
- Dr. Firman Leksmono SP - JP Basic ECG Interpretation For StudentDocument54 pagesDr. Firman Leksmono SP - JP Basic ECG Interpretation For Studentadela_97line100% (2)
- Revised AntiarrhythmicsDocument29 pagesRevised AntiarrhythmicsDang CuevasNo ratings yet
- Cvs PathoDocument36 pagesCvs PathoISRAELNo ratings yet
- Left and Right Heart Cath Procedure OverviewDocument43 pagesLeft and Right Heart Cath Procedure OverviewIr Soebagoes100% (2)
- Tissue Doppler ImagingDocument37 pagesTissue Doppler ImagingSruthiNo ratings yet
- The P WaveDocument13 pagesThe P Wave成失No ratings yet
- Right Heart Catheterization, NicvdDocument17 pagesRight Heart Catheterization, NicvdNavojit ChowdhuryNo ratings yet
- Pericardial Diseases 3rd Yr BMTDocument38 pagesPericardial Diseases 3rd Yr BMT211941103014100% (1)
- IHD CAUSES CHEST PAINDocument19 pagesIHD CAUSES CHEST PAINOsama MalikNo ratings yet
- Cardiomyopathy: Leonard Shaju Joisy AloorDocument34 pagesCardiomyopathy: Leonard Shaju Joisy AloorJoisy AloorNo ratings yet
- HBP C315HIS Implant Procedure-eLearnDocument35 pagesHBP C315HIS Implant Procedure-eLearnRichiNo ratings yet
- Basic EP IntervalsDocument13 pagesBasic EP IntervalsdrharoonmohdNo ratings yet
- DR K Chan - Ecg For SVT Made EasyDocument66 pagesDR K Chan - Ecg For SVT Made Easyapi-346486620No ratings yet
- ECG WorldDocument139 pagesECG WorldsatyaNo ratings yet
- Electrical Axis: Fast & Easy Ecgs - A Self-Paced Learning ProgramDocument29 pagesElectrical Axis: Fast & Easy Ecgs - A Self-Paced Learning ProgramMihaela PrisacaruNo ratings yet
- ECG ImportantDocument82 pagesECG ImportantAyyoob JafariNo ratings yet
- Cardiomyopathy Joisy AloorDocument31 pagesCardiomyopathy Joisy AloorJoisy AloorNo ratings yet
- 5 - Ventricular Tachyarrhythmias DoneDocument79 pages5 - Ventricular Tachyarrhythmias Doneclaimstudent3515No ratings yet
- BradyarrthmiaDocument73 pagesBradyarrthmiaKuba ArebaNo ratings yet
- Ecg Pathology 02Document95 pagesEcg Pathology 02Andi MP Manurung100% (1)
- Cardiovascular Nursing: Study Online atDocument7 pagesCardiovascular Nursing: Study Online atLilly DayeNo ratings yet
- Spectrum of Acute Coronary Syndrome: Milagros Estrada-Yamamoto, MDDocument62 pagesSpectrum of Acute Coronary Syndrome: Milagros Estrada-Yamamoto, MDAnonymous HH3c17osNo ratings yet
- Pulseless Electrical ActivityDocument2 pagesPulseless Electrical ActivitysrimatsimhasaneshwarNo ratings yet
- Study Frequency CounterDocument8 pagesStudy Frequency CounterMahadevNo ratings yet
- Cardiac Emergencies PDFDocument57 pagesCardiac Emergencies PDFJohn Paulo CatacutanNo ratings yet
- Mitral StenosisDocument50 pagesMitral Stenosissruthimeena6891No ratings yet
- Cardiac pacing guide for beginnersDocument89 pagesCardiac pacing guide for beginnerssandwhale056No ratings yet
- Cardiac DefibrillatorsDocument8 pagesCardiac Defibrillatorsصفا طلال نايفNo ratings yet
- Types and Management of Valvular Heart DiseaseDocument60 pagesTypes and Management of Valvular Heart DiseaseIntan Kumalasari RambeNo ratings yet
- 04 - Elements of EchocardiographyDocument56 pages04 - Elements of EchocardiographyMariana CabralNo ratings yet
- Heartbeat Irregularities ExplainedDocument5 pagesHeartbeat Irregularities ExplainedKayelyn-Rose Combate100% (1)
- CARDIAC CYCLE New For StudentDocument54 pagesCARDIAC CYCLE New For StudentDavi DzikirianNo ratings yet
- ECG LeadsDocument13 pagesECG LeadsPro fatherNo ratings yet
- Basic ECG Interpretation GuideDocument61 pagesBasic ECG Interpretation GuideHayat Hamzah DawiNo ratings yet
- Q: Characterize The Different Types of Pacemaker. Explain The Various Steps of PacingDocument4 pagesQ: Characterize The Different Types of Pacemaker. Explain The Various Steps of PacingKRUPALITHAKKAR100% (1)
- Cardiac Cycle: Mechanical Event and Their Electrical and Clinical CorrelationDocument28 pagesCardiac Cycle: Mechanical Event and Their Electrical and Clinical Correlationhawas muhammed100% (1)
- Heart Blood HistoDocument53 pagesHeart Blood HistoAnonymous 52lBinNo ratings yet
- Dysrhytmia NotesDocument11 pagesDysrhytmia NoteshannahhwolfNo ratings yet
- Atrial FlutterDocument38 pagesAtrial FlutterLady AngodNo ratings yet
- ATRIAL FIBRILLATION Anil KRDocument41 pagesATRIAL FIBRILLATION Anil KRanil sahNo ratings yet
- Managing Hypertension in PregnancyDocument8 pagesManaging Hypertension in PregnancyMuvenn KannanNo ratings yet
- Thoracic Trauma 980Document45 pagesThoracic Trauma 980Muvenn KannanNo ratings yet
- 6.examination of Inguinal SwellingDocument4 pages6.examination of Inguinal SwellingMuvenn Kannan100% (1)
- Cirrhosis 2 and SBPDocument56 pagesCirrhosis 2 and SBPMuvenn Kannan100% (1)
- Rheumatoid Arthritis MEQDocument3 pagesRheumatoid Arthritis MEQMuvenn KannanNo ratings yet
- Single Best Answer Emergency MedicienDocument11 pagesSingle Best Answer Emergency MedicienMuvenn Kannan100% (1)
- Advanced Trauma and Life Support (Atls) : by Anu Sandhya PG Ward 3Document34 pagesAdvanced Trauma and Life Support (Atls) : by Anu Sandhya PG Ward 3Muvenn KannanNo ratings yet
- Age Related Macular DegenerationDocument35 pagesAge Related Macular DegenerationMuvenn KannanNo ratings yet
- Meq 1 Paediatrics: Marks)Document4 pagesMeq 1 Paediatrics: Marks)Muvenn KannanNo ratings yet
- MEQ On BPPVDocument5 pagesMEQ On BPPVMuvenn KannanNo ratings yet
- Pyrexia of Unknown OriginDocument4 pagesPyrexia of Unknown OriginMuvenn KannanNo ratings yet
- Ospe 12Document2 pagesOspe 12Muvenn KannanNo ratings yet
- Pleural Effusion OSPEDocument2 pagesPleural Effusion OSPEMuvenn KannanNo ratings yet
- Gastric Carcinoma: H. Pylori InfectionDocument7 pagesGastric Carcinoma: H. Pylori InfectionMuvenn KannanNo ratings yet
- Intestinal Obstruction 3Document27 pagesIntestinal Obstruction 3Muvenn KannanNo ratings yet
- Organicbrainsyndrome 130619180626 Phpapp02Document46 pagesOrganicbrainsyndrome 130619180626 Phpapp02Muvenn KannanNo ratings yet
- Intestinal Obstruction 4Document25 pagesIntestinal Obstruction 4Muvenn KannanNo ratings yet
- Intestinal ObstructionDocument25 pagesIntestinal ObstructionMuvenn KannanNo ratings yet
- Fam 2 MCQDocument20 pagesFam 2 MCQMuvenn KannanNo ratings yet
- Intestinal Obstruction2Document26 pagesIntestinal Obstruction2TwinkleNo ratings yet
- Obs and Gynecology Placenta AcrretaDocument2 pagesObs and Gynecology Placenta AcrretaMuvenn KannanNo ratings yet
- ECG Changes in Chamber EnlargementDocument16 pagesECG Changes in Chamber EnlargementMuvenn KannanNo ratings yet
- Ocular Emergencies: Immediate TreatmentDocument86 pagesOcular Emergencies: Immediate TreatmentBenny Franclin SuripattyNo ratings yet
- Supervised wound procedures guideDocument50 pagesSupervised wound procedures guideMuvenn KannanNo ratings yet
- Enzymes Exam PaperDocument2 pagesEnzymes Exam PaperMuvenn KannanNo ratings yet
- Breastfeeding Benefits and Risks of JaundiceDocument81 pagesBreastfeeding Benefits and Risks of JaundiceMuvenn KannanNo ratings yet
- Biology Membrane ExamDocument9 pagesBiology Membrane ExamMuvenn KannanNo ratings yet
- Sed MmWave Sensor Series V2.0Document31 pagesSed MmWave Sensor Series V2.0snobic9379No ratings yet
- PHARMACOTHERAPEUTICS MCQSDocument17 pagesPHARMACOTHERAPEUTICS MCQSWwe 2No ratings yet
- Atrial Fibrillation-OfFICIALDocument13 pagesAtrial Fibrillation-OfFICIALChristelleMaeNo ratings yet
- Therapeutics Handbook 2014 - 140804Document384 pagesTherapeutics Handbook 2014 - 140804Eriet HidayatNo ratings yet
- Practice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaDocument28 pagesPractice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaRully SyahrizalNo ratings yet
- Amboss:CardioDocument18 pagesAmboss:CardioNicole Juliette CCNo ratings yet
- 2021 Abbott Annual ReportDocument86 pages2021 Abbott Annual ReportAdriano BolgenhagenNo ratings yet
- Hypertensive Heart Disease: A Proposed Clinical ClassificationDocument2 pagesHypertensive Heart Disease: A Proposed Clinical ClassificationireneaureliaNo ratings yet
- Acute Medicine 4th EdDocument660 pagesAcute Medicine 4th EdEmmanuel Ortiz100% (4)
- CABANADocument14 pagesCABANAIsmael Rivera DiazNo ratings yet
- IANs Presentation - Atrial Fibrillation (RMO Kerenga)Document26 pagesIANs Presentation - Atrial Fibrillation (RMO Kerenga)Samuel.MoriNo ratings yet
- Interventional Cardiology and SurgeryDocument19 pagesInterventional Cardiology and SurgeryDEV NANDHINI RNo ratings yet
- PLABABLEDocument25 pagesPLABABLESharith SilvaNo ratings yet
- RevisionDocument17 pagesRevisionMatt RenaudNo ratings yet
- Warfarin Patient Education and Adherence StrategiesDocument5 pagesWarfarin Patient Education and Adherence StrategiesJayson TrajanoNo ratings yet
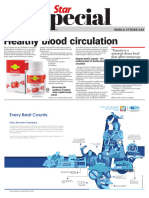
- World Stroke Day - 29 October 2023Document5 pagesWorld Stroke Day - 29 October 2023Times MediaNo ratings yet
- Anesthesia Guide for Mitral Stenosis PatientDocument67 pagesAnesthesia Guide for Mitral Stenosis PatientNamithaNo ratings yet
- Lecture Notes For SDAFP Family Medicine Update - 2012 PDFDocument305 pagesLecture Notes For SDAFP Family Medicine Update - 2012 PDFMaria MiripNo ratings yet
- Sbar Template RN To PDFDocument2 pagesSbar Template RN To PDFMichael StefanoNo ratings yet
- Ebstein's AnomalyDocument7 pagesEbstein's AnomalyRJMNo ratings yet
- ACLS Algorithms Adult 2010 Revised May 31 2011Document12 pagesACLS Algorithms Adult 2010 Revised May 31 2011arturschander3614No ratings yet
- Hemiplegia Resource Book ModifiedDocument60 pagesHemiplegia Resource Book ModifiedAnonymous czrvb3hNo ratings yet
- Report-Ecg Ctscan G3 Friday PDFDocument25 pagesReport-Ecg Ctscan G3 Friday PDFTrí Tạ MinhNo ratings yet
- Ambulatory ECG Monitoring in The Age of SmartphonesDocument11 pagesAmbulatory ECG Monitoring in The Age of SmartphonesSaul PeñaNo ratings yet
- The Impact of Coffee Subtypes On Incident Cardiovascular Disease, Arrhythmias, and MortalityDocument10 pagesThe Impact of Coffee Subtypes On Incident Cardiovascular Disease, Arrhythmias, and MortalityJenny RojoNo ratings yet
- Efficacy and Safety o A Dedicated LAAO Protocol 2022Document3 pagesEfficacy and Safety o A Dedicated LAAO Protocol 2022吳醫師No ratings yet
- Cardioembolic StrokeDocument20 pagesCardioembolic StrokeEdwinda Desy Ratu100% (1)
- NeurocardiologyDocument2 pagesNeurocardiologybala1307No ratings yet