You might also like
- Prac SigDocument26 pagesPrac SigTanvir AhmedNo ratings yet
- Tramadol Seizure ThresholdDocument2 pagesTramadol Seizure ThresholdTanvir AhmedNo ratings yet
- Urinary Incontinence Causes and TreatmentDocument5 pagesUrinary Incontinence Causes and TreatmentTanvir AhmedNo ratings yet
- 35321Document22 pages35321Viinaviino IiaaiiaaooNo ratings yet
- 9 GlycogenDocument37 pages9 GlycogenShendi SuryanaNo ratings yet
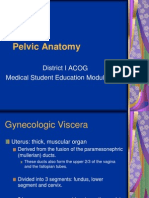
- Pelvic AnatomyDocument23 pagesPelvic AnatomyYudhi AuliaNo ratings yet
- Membrane-Binding Mechanism of Clostridium Perfringens Alpha-ToxinDocument8 pagesMembrane-Binding Mechanism of Clostridium Perfringens Alpha-ToxinTanvir AhmedNo ratings yet
- 5.-Brainstem Han 2015Document32 pages5.-Brainstem Han 2015Tanvir AhmedNo ratings yet
- FootworkDocument1 pageFootworkTanvir AhmedNo ratings yet
- Cerebellum 1Document1 pageCerebellum 1Tanvir AhmedNo ratings yet
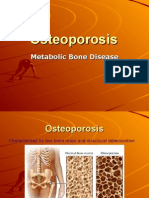
- Osteo Ma Laci A OsteoporosisDocument28 pagesOsteo Ma Laci A OsteoporosislouradelNo ratings yet
- SphingolipidosesDocument8 pagesSphingolipidosesTanvir AhmedNo ratings yet
- DNA Rep AirDocument23 pagesDNA Rep AirTanvir AhmedNo ratings yet
- What Is Biochemistry NBME USMLE ABCDDocument37 pagesWhat Is Biochemistry NBME USMLE ABCDTanvir Ahmed100% (1)
- IschemiaDocument81 pagesIschemiaTanvir AhmedNo ratings yet
- Nursing ProfessionalisminNursing 1Document7 pagesNursing ProfessionalisminNursing 1Tanvir AhmedNo ratings yet
- 5.-Brainstem Han 2015Document32 pages5.-Brainstem Han 2015Tanvir AhmedNo ratings yet
- CardiomyopathiesDocument48 pagesCardiomyopathiesTanvir AhmedNo ratings yet
- Osteo Ma Laci A OsteoporosisDocument28 pagesOsteo Ma Laci A OsteoporosislouradelNo ratings yet
- Compilation NBME NeuroDocument3 pagesCompilation NBME NeuroTanvir AhmedNo ratings yet
- Goljan Audio TranscriptDocument234 pagesGoljan Audio TranscriptHuan Bien100% (4)
- 9 GlycogenDocument37 pages9 GlycogenShendi SuryanaNo ratings yet
- SoapDocument5 pagesSoapallele940% (1)
- Diagnosing Pneumonia by History and PhysicalDocument3 pagesDiagnosing Pneumonia by History and PhysicalTanvir AhmedNo ratings yet
- IschemiaDocument81 pagesIschemiaTanvir AhmedNo ratings yet
- Thalamus NotesDocument11 pagesThalamus NotesTanvir AhmedNo ratings yet
- SlaveryDocument1 pageSlaveryTanvir AhmedNo ratings yet
- SlaveryDocument1 pageSlaveryTanvir AhmedNo ratings yet
- Autonomic Nervous System PharmacologyDocument13 pagesAutonomic Nervous System PharmacologySam BotNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Treatment of Rheumatoid Arthritis in Patients With Concomitant Chronic Hepatitis C InfectionDocument24 pagesTreatment of Rheumatoid Arthritis in Patients With Concomitant Chronic Hepatitis C InfectionMuhammad Farras Razin PerdanaNo ratings yet
- JMedLife 16 195Document8 pagesJMedLife 16 195Victoria VelardeNo ratings yet
- Red Eyes Guide: Causes and TreatmentsDocument45 pagesRed Eyes Guide: Causes and TreatmentsDavidVictoriousLukas100% (1)
- EpiDocument3 pagesEpiNiño PaoloNo ratings yet
- Ebola Virus Disease: 39. 40. Good Luck and God Bless!Document1 pageEbola Virus Disease: 39. 40. Good Luck and God Bless!Bobet ReñaNo ratings yet
- Common Childhood Diseases and Healthy HabitsDocument6 pagesCommon Childhood Diseases and Healthy HabitsHF ManigbasNo ratings yet
- B. Natural History of Disease WorksheetDocument3 pagesB. Natural History of Disease WorksheetYahya MoralesNo ratings yet
- Blood Anatomy and Physiology: Functions, Components, Groups, and TypingDocument28 pagesBlood Anatomy and Physiology: Functions, Components, Groups, and TypingPORTRAIT OF A NURSENo ratings yet
- E-Poster Enterics For Global Health Shigella Surveillance StudyDocument1 pageE-Poster Enterics For Global Health Shigella Surveillance StudyNeyama AlladinNo ratings yet
- Viral Diseases MechanismsDocument105 pagesViral Diseases MechanismspolypeptideNo ratings yet
- Lab Report Provides Accurate CBC ResultsDocument1 pageLab Report Provides Accurate CBC ResultsHafiz GurjarNo ratings yet
- Pemphigoid Gestationis Update May 2017 - Lay Review March 2017Document4 pagesPemphigoid Gestationis Update May 2017 - Lay Review March 2017Andrei MurariuNo ratings yet
- Vaccination in PregnancyDocument7 pagesVaccination in PregnancyNoraNo ratings yet
- English Essay Topics on COVID-19 PandemicDocument4 pagesEnglish Essay Topics on COVID-19 Pandemicmaria evangelistaNo ratings yet
- Untitled21 PDFDocument18 pagesUntitled21 PDFElizabeth LeonNo ratings yet
- Tuberculin Skin TestingDocument4 pagesTuberculin Skin Testingmick saNo ratings yet
- SalmonellaDocument14 pagesSalmonelladrparachuruNo ratings yet
- Effect of BCG Vaccination Against Mycobacterium: Tuberculosis Infection in ChildrenDocument2 pagesEffect of BCG Vaccination Against Mycobacterium: Tuberculosis Infection in ChildrennissieNo ratings yet
- BC Lioton SKDocument71 pagesBC Lioton SKAlejandra Cale Radowitz0% (1)
- Kit InsertDocument8 pagesKit InsertMuhammad HamzarNo ratings yet
- Evidence-Based Guideline: Clinical Evaluation and Treatment of Transverse MyelitisDocument8 pagesEvidence-Based Guideline: Clinical Evaluation and Treatment of Transverse MyelitisAnonymous V5l8nmcSxbNo ratings yet
- UTF-8''diarrhea 13-11-13Document32 pagesUTF-8''diarrhea 13-11-13yoga yogafenkanoNo ratings yet
- Janeway's Immunobiology 8thDocument892 pagesJaneway's Immunobiology 8thSergio Falcon Rivera92% (12)
- Hav Igm CTKDocument2 pagesHav Igm CTKGu AleXanderNo ratings yet
- 9 Th. Lec. Lewis Blood Group SystemDocument11 pages9 Th. Lec. Lewis Blood Group Systemda202263357026No ratings yet
- Respiratory Tract InfectionsDocument17 pagesRespiratory Tract InfectionsPriya bhattiNo ratings yet
- Form Lab RSBM NewDocument2 pagesForm Lab RSBM NewKiki OlivianaNo ratings yet
- CDC Guidelines on Standard and Transmission-Based PrecautionsDocument6 pagesCDC Guidelines on Standard and Transmission-Based PrecautionsKomite PPI RSUDPCNo ratings yet
- FINAL EXAM RSUD CENGKARENG JawabDocument17 pagesFINAL EXAM RSUD CENGKARENG JawabSyah TrianaNo ratings yet
- Antihbe ArcDocument7 pagesAntihbe Arctesteste testeNo ratings yet