You might also like
- TEAM Slides - 3rd EditionDocument77 pagesTEAM Slides - 3rd EditionCoass 82100% (1)
- Initial Assessment and Management Initial Assessment and ManagementDocument6 pagesInitial Assessment and Management Initial Assessment and Managementjc_sibal13No ratings yet
- Initial Assessment and Management of Multiply Injured PatientsDocument30 pagesInitial Assessment and Management of Multiply Injured PatientsSikaNo ratings yet
- EN Primary SurveyDocument32 pagesEN Primary SurveythoriqNo ratings yet
- Airway AdjunctsDocument17 pagesAirway AdjunctsChannelGNo ratings yet
- Primary Trauma CareDocument48 pagesPrimary Trauma CareKABERA RENENo ratings yet
- Patient Safety: Early Warning ScoreDocument50 pagesPatient Safety: Early Warning ScoreAiko himeNo ratings yet
- General Surgery 27-03-07Document7 pagesGeneral Surgery 27-03-07Raghu VeerNo ratings yet
- 7 Steps Patient SafetyDocument58 pages7 Steps Patient SafetyDanissa Fidia PuteriNo ratings yet
- Management of Multiple Traumatised PatientDocument4 pagesManagement of Multiple Traumatised PatientOmar MohammedNo ratings yet
- Neb Ul IzationDocument15 pagesNeb Ul IzationhoohooNo ratings yet
- DialysisDocument20 pagesDialysisSiwani rai100% (1)
- Peadiatric Brain Tumour: Wong Ann Cheng MD (Ukm) MRCPCH (Uk)Document48 pagesPeadiatric Brain Tumour: Wong Ann Cheng MD (Ukm) MRCPCH (Uk)An Zheng100% (4)
- Upper Airway Anatomy and FunctionDocument86 pagesUpper Airway Anatomy and FunctionekaefkaNo ratings yet
- Trauma and Emergency NursingDocument9 pagesTrauma and Emergency Nursingchinthaka18389021No ratings yet
- Nasal Fractures: Trauma To NoseDocument38 pagesNasal Fractures: Trauma To NoseSindhura ManjunathNo ratings yet
- BRONCHIOLITIS CARE GUIDEDocument22 pagesBRONCHIOLITIS CARE GUIDEAlfani FajarNo ratings yet
- Post Antibiotic Era Emerging Concern To HumanityDocument47 pagesPost Antibiotic Era Emerging Concern To Humanitytummalapalli venkateswara raoNo ratings yet
- Cardiac TamponadeDocument18 pagesCardiac Tamponadeyelsinosmin romeroalvaradoNo ratings yet
- Introduction To Patient SafetyDocument54 pagesIntroduction To Patient Safetyrejoicedear2020No ratings yet
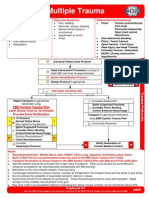
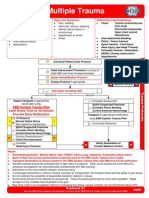
- Multiple Trauma ManagementDocument1 pageMultiple Trauma ManagementSetiawan Arif WibowoNo ratings yet
- ABCs of Thoracic TraumaDocument5 pagesABCs of Thoracic TraumaAlice S ChangNo ratings yet
- Torso TraumaDocument58 pagesTorso TraumaAbidisHereNo ratings yet
- Respiratory Emergencies2Document47 pagesRespiratory Emergencies2yeniNo ratings yet
- Laryngeal ObstructionDocument59 pagesLaryngeal ObstructionpravinNo ratings yet
- Preoperative Assessment ChecklistDocument27 pagesPreoperative Assessment ChecklistHairina MazlanNo ratings yet
- Topic Congenital PneumoniaDocument11 pagesTopic Congenital PneumoniaPomtungNo ratings yet
- Hydranencephaly ManagementDocument20 pagesHydranencephaly ManagementJohn Christopher LucesNo ratings yet
- Chin lift/jaw thrust• Insertion of oropharyngeal airwayDocument39 pagesChin lift/jaw thrust• Insertion of oropharyngeal airwayDiajengMaria'benedictaOctavianiOsokPrasetyoNo ratings yet
- 10.08.07 Cardiac Tamponade HaagDocument16 pages10.08.07 Cardiac Tamponade HaagfoetorNo ratings yet
- Dr. SK Mathur High Flow Nasal Oxygen TherapyDocument20 pagesDr. SK Mathur High Flow Nasal Oxygen TherapyAnish H Dave100% (1)
- In Partial Fulfillment of The Requirements in Strategies in Health EducationDocument11 pagesIn Partial Fulfillment of The Requirements in Strategies in Health EducationEduardNo ratings yet
- Management of Hypoxia During AnaesthesiaDocument5 pagesManagement of Hypoxia During AnaesthesiaNurhafizahImfista100% (1)
- Cardiac Tamponade: Signs, Symptoms and DiagnosisDocument20 pagesCardiac Tamponade: Signs, Symptoms and Diagnosismuhammad iqbal mahfuzhNo ratings yet
- Congenital SyphilisDocument3 pagesCongenital SyphilisadmusNo ratings yet
- Newborn ResuscitationDocument57 pagesNewborn ResuscitationmateenNo ratings yet
- Cataract Surgery ProtocolsDocument17 pagesCataract Surgery ProtocolsRahul ShastriNo ratings yet
- Asthma Proper Nebulization TechniqueDocument2 pagesAsthma Proper Nebulization Techniquejhamz_21No ratings yet
- Salbutamol AcidosisDocument3 pagesSalbutamol AcidosisAccounts OfficerNo ratings yet
- Causes and Management of Syncope in DentistryDocument27 pagesCauses and Management of Syncope in DentistrySelvarathi KandhaswamyNo ratings yet
- Status EpilepticusDocument70 pagesStatus Epilepticusfloppyfishh100% (1)
- Uhns Guidelines 2010Document187 pagesUhns Guidelines 2010varrakesh100% (1)
- Nephrotic SyndromeDocument14 pagesNephrotic SyndromeAnna Michael AbdullahNo ratings yet
- Thalassemia: Dr. Deep Shah Under Guidance of Dr. Krutika Ma'Am and Dr. Rahul SirDocument46 pagesThalassemia: Dr. Deep Shah Under Guidance of Dr. Krutika Ma'Am and Dr. Rahul SirDeep ShahNo ratings yet
- Allergic Rhinitis in Children: A Common but Treatable ConditionDocument7 pagesAllergic Rhinitis in Children: A Common but Treatable ConditionTina MorleyNo ratings yet
- Early Warning Score & Rapid Response TeamDocument26 pagesEarly Warning Score & Rapid Response TeamAsim IdreesNo ratings yet
- Amblyopia: Glomarie Hope A. Paquera Danica Ilah M. SincoDocument39 pagesAmblyopia: Glomarie Hope A. Paquera Danica Ilah M. SincoJan IrishNo ratings yet
- Nebulization SHODocument10 pagesNebulization SHOkotekingNo ratings yet
- The Science Behind NRP 7th EditionDocument45 pagesThe Science Behind NRP 7th Editionviaerea100% (1)
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocument1 pageMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonNo ratings yet
- A Neonate With Acute Kidney Injury: Case PresentationDocument4 pagesA Neonate With Acute Kidney Injury: Case PresentationSahil DhamijaNo ratings yet
- Advanced AirwayDocument34 pagesAdvanced Airwayvica_christiaNo ratings yet
- Laboratory Diagnosis of Infectious Diseases GuidelineDocument100 pagesLaboratory Diagnosis of Infectious Diseases GuidelineGalo PinosNo ratings yet
- K1 - Initial AssessmentDocument34 pagesK1 - Initial Assessmentpuja argaNo ratings yet
- ATLS: Initial Assessment and Management: SAUSHEC Medical Student Lecture SeriesDocument52 pagesATLS: Initial Assessment and Management: SAUSHEC Medical Student Lecture SeriesAndrew SuryaNo ratings yet
- Initial Assessment and ManagementDocument47 pagesInitial Assessment and Managementrazan asadNo ratings yet
- ATLSDocument52 pagesATLSBelLa EakoiNo ratings yet
- TraumaDocument2 pagesTraumajc_sibal13No ratings yet
- Primary Survey in Trauma PatientsDocument37 pagesPrimary Survey in Trauma PatientsJaismi AntonyNo ratings yet
- 7.down SyndromeDocument15 pages7.down SyndromeGadarNo ratings yet
- GD3. Normal ChildOKDocument22 pagesGD3. Normal ChildOKArinta AtmasariNo ratings yet
- 7.down SyndromeDocument15 pages7.down SyndromeGadarNo ratings yet
- Present SmotheringDocument19 pagesPresent SmotheringRagil SludgeMetal FtdNo ratings yet
- Konstribusi Islam Dalam Kedokteran Modern: Prof - Dr.Eddy Mart Salim, SPPD, K-AiDocument27 pagesKonstribusi Islam Dalam Kedokteran Modern: Prof - Dr.Eddy Mart Salim, SPPD, K-AiGadarNo ratings yet
- Neonatal SeizureDocument36 pagesNeonatal SeizurelovablemomNo ratings yet
- Scald Injury Educator's GuideDocument20 pagesScald Injury Educator's Guidetutor tujuhNo ratings yet
- Case Control LegDocument33 pagesCase Control LegGadarNo ratings yet
- Paraprhasing, Sitasi Dan Daftar PustakaDocument43 pagesParaprhasing, Sitasi Dan Daftar PustakaGadarNo ratings yet
- Case SeriesDocument19 pagesCase SeriesdesioktarianaNo ratings yet
- Frostbite: ConsiderationsDocument3 pagesFrostbite: ConsiderationsGadarNo ratings yet
- A Guide Quasi Experiment DesignsDocument11 pagesA Guide Quasi Experiment DesignsGadarNo ratings yet
- Cross Sectional StudyDocument49 pagesCross Sectional StudyGadarNo ratings yet
- Cross Sectional Red BullDocument53 pagesCross Sectional Red BulldesioktarianaNo ratings yet
- Cohort Study LegDocument23 pagesCohort Study LegGadarNo ratings yet
- Neonatal HyperbilirubinemiaDocument63 pagesNeonatal HyperbilirubinemiaGadarNo ratings yet
- Pedoman Nasional Etik Penelitian KesehatanDocument43 pagesPedoman Nasional Etik Penelitian KesehatanGadarNo ratings yet
- Asphyxia Neonatorum Diagnosis, Risk Factors and ManagementDocument35 pagesAsphyxia Neonatorum Diagnosis, Risk Factors and ManagementMuhammad RagilNo ratings yet
- Halaman Logo Per BabDocument1 pageHalaman Logo Per BabGadarNo ratings yet
- Neonatal HyperbilirubinemiaDocument63 pagesNeonatal HyperbilirubinemiaGadarNo ratings yet
- Neonatal InfectionDocument56 pagesNeonatal InfectionAgust SalimNo ratings yet
- The Low Birth Weight Infant: Julniar M Tasli Herman BermawiDocument42 pagesThe Low Birth Weight Infant: Julniar M Tasli Herman BermawiJoNo ratings yet
- PONV 30 Mar 2010 AmitDocument46 pagesPONV 30 Mar 2010 AmitAmit KochetaNo ratings yet
- Marie Perez Case StudyDocument1 pageMarie Perez Case StudyJohn Wick100% (1)
- The Jordan Peterson Meat-Only Diet - The AtlanticDocument1 pageThe Jordan Peterson Meat-Only Diet - The AtlanticMaciej PogorzelskiNo ratings yet
- Therapeutic Protocol of Paleomedicina HungaryDocument2 pagesTherapeutic Protocol of Paleomedicina HungaryzC6MuNiWNo ratings yet
- CirculationDocument14 pagesCirculationEsteban Martin Chiotti KaneshimaNo ratings yet
- Maternity and Women's Health Care 11th Edition Lowdermilk Test BankDocument12 pagesMaternity and Women's Health Care 11th Edition Lowdermilk Test BankAlex0% (1)
- AIIMS Jodhpur Faculty Recruitment Result 2019Document2 pagesAIIMS Jodhpur Faculty Recruitment Result 2019Mega CreationsNo ratings yet
- Approach To Mast Cell Activation SyndromeDocument15 pagesApproach To Mast Cell Activation SyndromeKiki sNo ratings yet
- Beta Lactams Macrolides: ST ND THDocument5 pagesBeta Lactams Macrolides: ST ND THRheenz FornolesNo ratings yet
- Eat - Sleep - BurnDocument36 pagesEat - Sleep - BurnIt's Just MeNo ratings yet
- Classification of Pulpal & Periapical PathosisDocument51 pagesClassification of Pulpal & Periapical PathosismegamarwaNo ratings yet
- J Cellular Molecular Medi - 2014 - Liu - The Multiple Functional Roles of Mesenchymal Stem Cells in Participating inDocument10 pagesJ Cellular Molecular Medi - 2014 - Liu - The Multiple Functional Roles of Mesenchymal Stem Cells in Participating indr. RiyanNo ratings yet
- Dr. Ron P. GallemoreDocument2 pagesDr. Ron P. GallemoredrgallemoreaNo ratings yet
- Pharmacology of Catecholamines and Non-Catecholamines in ANSDocument6 pagesPharmacology of Catecholamines and Non-Catecholamines in ANSAmaetenNo ratings yet
- History Taking in PaediatricsDocument24 pagesHistory Taking in PaediatricsphilipNo ratings yet
- c-ANCA ELISADocument2 pagesc-ANCA ELISAYousra ZeidanNo ratings yet
- Juvenile Idiopathic ArthritisDocument52 pagesJuvenile Idiopathic ArthritishasanajNo ratings yet
- Dka Case StudyDocument3 pagesDka Case StudyMaryjoy Gabriellee De La CruzNo ratings yet
- Siu Yuen Surgery Notes PDFDocument213 pagesSiu Yuen Surgery Notes PDFAnonymous w4lLoMd7100% (1)
- Requirements for European Class 3 Medical Certification of Air Traffic ControllersDocument56 pagesRequirements for European Class 3 Medical Certification of Air Traffic ControllersmalidalkiranNo ratings yet
- Recent Updates On Nanomedicine Based Products: Current Sce-Nario and Future OpportunitiesDocument13 pagesRecent Updates On Nanomedicine Based Products: Current Sce-Nario and Future OpportunitiesvijuNo ratings yet
- Chapter 15: The Gastrointestinal System: Multiple Choice. Choose The Correct AnswerDocument3 pagesChapter 15: The Gastrointestinal System: Multiple Choice. Choose The Correct AnswerbillyNo ratings yet
- Assessment Subjective: " Hindi Ako Makatulog KapagDocument4 pagesAssessment Subjective: " Hindi Ako Makatulog KapagrholiboiNo ratings yet
- ThiazolidinedioneDocument9 pagesThiazolidinedioneadyaly44No ratings yet
- Updates in Management of Enterocutaneous FistulaDocument35 pagesUpdates in Management of Enterocutaneous FistulabashiruNo ratings yet
- Herb BookDocument32 pagesHerb Bookbroodhunter2No ratings yet
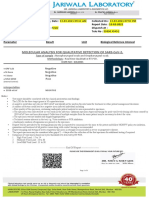
- Molecular Analysis For Qualitative Detection of Sars-Cov-2.: Negative Negative Negative PassDocument4 pagesMolecular Analysis For Qualitative Detection of Sars-Cov-2.: Negative Negative Negative PassmeezNo ratings yet
- Oregano Oil Kills E. coli & P. aeruginosaDocument2 pagesOregano Oil Kills E. coli & P. aeruginosaRadomir BoljevicNo ratings yet
- DRUG STUDY Magnesium SulfateDocument4 pagesDRUG STUDY Magnesium SulfateTempoNo ratings yet