You might also like
- Case Report OsteochondromaDocument43 pagesCase Report OsteochondromaFidesha Nurganiah SiregarNo ratings yet
- Radio Logical Assessment of OA FinalDocument60 pagesRadio Logical Assessment of OA FinaltarikeopsNo ratings yet
- Giant Cell Tumor: MUH - YUSUF M C11111 893 NURHIDAYAH C11111 120 Yoriche Tallamma C11111 293 Andi Nirmawati. Ar C11112 063Document34 pagesGiant Cell Tumor: MUH - YUSUF M C11111 893 NURHIDAYAH C11111 120 Yoriche Tallamma C11111 293 Andi Nirmawati. Ar C11112 063AndinNo ratings yet
- Presentasi Radiologi: Dita Ayu Pertiwi FAA 114 016Document88 pagesPresentasi Radiologi: Dita Ayu Pertiwi FAA 114 016dita ayuNo ratings yet
- Casereports 3 1083Document4 pagesCasereports 3 1083nadila raudhani pNo ratings yet
- OA - Ahmad Aulia Rizaly - DR Andry Usman SpOTDocument34 pagesOA - Ahmad Aulia Rizaly - DR Andry Usman SpOTNur Syamsiah MNo ratings yet
- Osteoarthritis 191016103144Document49 pagesOsteoarthritis 191016103144dr.abouzaid098No ratings yet
- Open Fracture 1/3 Distal Right Fibula Grade Iiib Open Fracture Segmental Right Tibia Grade IiibDocument24 pagesOpen Fracture 1/3 Distal Right Fibula Grade Iiib Open Fracture Segmental Right Tibia Grade IiibDokter muda BedahNo ratings yet
- Myth-Busting Facts About OsteoarthritisDocument17 pagesMyth-Busting Facts About OsteoarthritisMuskan khaziNo ratings yet
- Introduction to Osteoarthritis: Causes, Symptoms and TreatmentDocument39 pagesIntroduction to Osteoarthritis: Causes, Symptoms and TreatmentSri MahadhanaNo ratings yet
- Osteo Arthit IsDocument19 pagesOsteo Arthit IsShaa ShawalishaNo ratings yet
- APLEY & SOLOMON'S - 5. OsteoarthritisDocument19 pagesAPLEY & SOLOMON'S - 5. OsteoarthritisOngko SetunggalNo ratings yet
- 1-22 Osteoporosis & Hip PainDocument79 pages1-22 Osteoporosis & Hip PaintarikeopsNo ratings yet
- Osteoarthritis: (Degenerative Arthritis/osteoarthrosis/hypertrophic Arthritis)Document64 pagesOsteoarthritis: (Degenerative Arthritis/osteoarthrosis/hypertrophic Arthritis)Linda SugiartoNo ratings yet
- Ra and Osteoarthritis R IfDocument43 pagesRa and Osteoarthritis R IfsnfhanNo ratings yet
- Disorders of The Foot and Leg ConfDocument304 pagesDisorders of The Foot and Leg ConfhaminatrafNo ratings yet
- Algodystrophy (AD) : Prof. Hazem Abdel Azeem (MD)Document179 pagesAlgodystrophy (AD) : Prof. Hazem Abdel Azeem (MD)tarikeopsNo ratings yet
- Trauma - Intertrochanteric Fracture - RustiniDocument7 pagesTrauma - Intertrochanteric Fracture - Rustinidedyalkarni08No ratings yet
- Case FractureDocument40 pagesCase FractureNidhia BadjakNo ratings yet
- Case Presentation: Ostheoarthtritis of KneeDocument31 pagesCase Presentation: Ostheoarthtritis of KneemarindadaNo ratings yet
- Case Report OADocument31 pagesCase Report OAmarindadaNo ratings yet
- Laporan Kasus MELORHEOSTOSISDocument54 pagesLaporan Kasus MELORHEOSTOSISEliana MuisNo ratings yet
- Update A1 OsceDocument120 pagesUpdate A1 OsceIndra SetyaNo ratings yet
- Nursing Care For Patients Undergoing Total Hip Arthroplasty: December 2018Document13 pagesNursing Care For Patients Undergoing Total Hip Arthroplasty: December 2018Stella GašparušNo ratings yet
- Osteoarthritis and InflammatoryDocument58 pagesOsteoarthritis and InflammatoryAfifah SelamatNo ratings yet
- Osteoid Osteoma of The Mandible: January 2014Document7 pagesOsteoid Osteoma of The Mandible: January 2014wirda yunita darwisNo ratings yet
- ARTHRITIS TB KNEE HIP BPTDocument84 pagesARTHRITIS TB KNEE HIP BPTMiso100% (1)
- Osteoarthritis & Gouty ArthritisDocument94 pagesOsteoarthritis & Gouty ArthritisStar CruiseNo ratings yet
- Giant Cell Tumor of Bone: Case ReportDocument36 pagesGiant Cell Tumor of Bone: Case ReportIndra ChristiantoNo ratings yet
- ARTHRITISDocument4 pagesARTHRITISJk FloresNo ratings yet
- Degenerative Sport (Autosaved)Document71 pagesDegenerative Sport (Autosaved)Elisabeth Permatasari SidabutarNo ratings yet
- Inflammatory Joint Diseases Handout-Admission ExamDocument11 pagesInflammatory Joint Diseases Handout-Admission ExamNona NadimNo ratings yet
- Osteoarthritis AapmrDocument5 pagesOsteoarthritis AapmrBiandaNo ratings yet
- p3 MusketDocument39 pagesp3 MusketAde Cahyo IslamiNo ratings yet
- Closed Tibia and Fibula Fracture Case PresentationDocument30 pagesClosed Tibia and Fibula Fracture Case Presentationzhafran_darwisNo ratings yet
- ArthritisDocument20 pagesArthritisPdianghunNo ratings yet
- Rheumatoid ArthritisDocument30 pagesRheumatoid ArthritisMelisaNo ratings yet
- Open Fracture 1/3 Middle Femur Sinistra: Case ReportDocument30 pagesOpen Fracture 1/3 Middle Femur Sinistra: Case ReportAnggita Efipania Silambi'No ratings yet
- Case Report: Osteoarthritis: Mutiara Riahna Sitepu 030.12.179 Pembimbing Dr. T. Nurrobi, SP - OT (K) HandDocument50 pagesCase Report: Osteoarthritis: Mutiara Riahna Sitepu 030.12.179 Pembimbing Dr. T. Nurrobi, SP - OT (K) Handmutiara sitepuNo ratings yet
- Severe Pain and Swelling in Left Leg After Traffic AccidentDocument37 pagesSevere Pain and Swelling in Left Leg After Traffic AccidentAde Cahyo IslamiNo ratings yet
- Dr. Md. Golam SarwarDocument41 pagesDr. Md. Golam Sarwarapi-26362375No ratings yet
- OsteoarthritisDocument39 pagesOsteoarthritisRohit RajeevNo ratings yet
- Bone Healing and Non UnionsDocument50 pagesBone Healing and Non UnionsFelicia BockNo ratings yet
- Lipoma, The Universal Tumor: in A Rare Location: Case ReportDocument4 pagesLipoma, The Universal Tumor: in A Rare Location: Case ReportWahyudi DobonsoloNo ratings yet
- Bedah 2 Mei 2019 PDFDocument210 pagesBedah 2 Mei 2019 PDFRinto MangiwaNo ratings yet
- Managing Open FracturesDocument256 pagesManaging Open FracturesZhraaNo ratings yet
- Treating a Closed Supracondylar Fracture of the Right FemurDocument37 pagesTreating a Closed Supracondylar Fracture of the Right FemurSri Mahtufa Riski100% (1)
- Defining Arthritis: Arth + It IsDocument82 pagesDefining Arthritis: Arth + It IsRofi IrmanNo ratings yet
- Common CasesDocument44 pagesCommon CasesRebecca WongNo ratings yet
- HNP CervicalDocument33 pagesHNP CervicalIndra RanteNo ratings yet
- Colles FractureDocument89 pagesColles Fracturenur syafiqah kamaruzaman100% (1)
- Advisor: DR - Padlan DR - Luthf Supervisor: Dr. Notinas Horas, M.Kes, SP - OT Orthopaedic and Traumatology DepartmentDocument34 pagesAdvisor: DR - Padlan DR - Luthf Supervisor: Dr. Notinas Horas, M.Kes, SP - OT Orthopaedic and Traumatology DepartmentroserosannaNo ratings yet
- 6 Kuliah Radiology of MSKDocument46 pages6 Kuliah Radiology of MSKDesak PratiwiNo ratings yet
- Radiology in ArthritisDocument96 pagesRadiology in Arthritissushrit neelopantNo ratings yet
- Osteonecrosis Caput FemurDocument23 pagesOsteonecrosis Caput FemurdrhendyjuniorNo ratings yet
- Amputation - DR EKADocument41 pagesAmputation - DR EKADiah agungNo ratings yet
- Osteoarthritis & Rheumatoid ArthritisDocument60 pagesOsteoarthritis & Rheumatoid ArthritisSaya MenangNo ratings yet
- Case Report (Ola)Document44 pagesCase Report (Ola)amel015No ratings yet
- Radioanatomy of The Extremities & Some of The MSK PathologiesDocument114 pagesRadioanatomy of The Extremities & Some of The MSK PathologiesTogodly 07No ratings yet
- Perspectives On Large Bowel Obstruction: January 2017Document5 pagesPerspectives On Large Bowel Obstruction: January 2017JeadeNo ratings yet
- LBOODocument10 pagesLBOOJeadeNo ratings yet
- RDocument48 pagesRJeadeNo ratings yet
- Ostearthritis Knee: Dr. Andry Usman, PH.D, SP - OT (K)Document42 pagesOstearthritis Knee: Dr. Andry Usman, PH.D, SP - OT (K)JeadeNo ratings yet
- Ostearthritis Knee: Dr. Andry Usman, PH.D, SP - OT (K)Document42 pagesOstearthritis Knee: Dr. Andry Usman, PH.D, SP - OT (K)JeadeNo ratings yet
- Ostearthritis Knee: Dr. Andry Usman, PH.D, SP - OT (K)Document42 pagesOstearthritis Knee: Dr. Andry Usman, PH.D, SP - OT (K)JeadeNo ratings yet
- Fisiologi Mata: Raja Muhammad Syafiq Bin Raja Azman C11113841Document21 pagesFisiologi Mata: Raja Muhammad Syafiq Bin Raja Azman C11113841JeadeNo ratings yet
- HFGVDocument3 pagesHFGVJeadeNo ratings yet
- Ostearthritis Knee: Dr. Andry Usman, PH.D, SP - OT (K)Document42 pagesOstearthritis Knee: Dr. Andry Usman, PH.D, SP - OT (K)JeadeNo ratings yet
- Andi MahmudDocument5 pagesAndi MahmudJeadeNo ratings yet
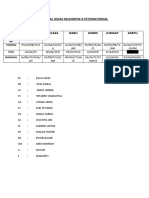
- Jadwal Dinas Kelompok FetomaternalDocument1 pageJadwal Dinas Kelompok FetomaternalJeadeNo ratings yet
- Andi MahmudDocument5 pagesAndi MahmudJeadeNo ratings yet
- Zeoreport - ZeolitaDocument17 pagesZeoreport - ZeolitageofloNo ratings yet
- Cancer massage therapy contraindicationsDocument15 pagesCancer massage therapy contraindicationsMya AlissandraNo ratings yet
- TNT - Terapia de Nutricion TotalDocument6 pagesTNT - Terapia de Nutricion TotalJuana Rosa Martinez BonillaNo ratings yet
- Aluminium SmelterDocument9 pagesAluminium SmelterAnup Dalal100% (1)
- Material Safety Data Sheet: 1. Product and Company IdentificationDocument9 pagesMaterial Safety Data Sheet: 1. Product and Company IdentificationAdeNo ratings yet
- Nutrients 10 01103 v2Document21 pagesNutrients 10 01103 v2Ida Ayu LitaNo ratings yet
- Mola Hidantidosa & Gestational Trophoblastic NeoplasmaDocument23 pagesMola Hidantidosa & Gestational Trophoblastic NeoplasmanurkamilawatiNo ratings yet
- Expert Committee On The Diagnosis and Classification of Diabetes (2003) PDFDocument16 pagesExpert Committee On The Diagnosis and Classification of Diabetes (2003) PDFPattyNo ratings yet
- Internal Medicine - DermatologyDocument125 pagesInternal Medicine - DermatologySoleil DaddouNo ratings yet
- Pleural DiseasesDocument4 pagesPleural DiseasesJennifer DayNo ratings yet
- Jake's PrognosisDocument3 pagesJake's PrognosisSiegNo ratings yet
- Soal 1Document7 pagesSoal 1GABRIELAW ANGELIKANo ratings yet
- BSGAR Interesting Case PresentationDocument7 pagesBSGAR Interesting Case PresentationMa. Soledad RodriguezNo ratings yet
- Autoimmune Disease - Why and Where It OccursDocument7 pagesAutoimmune Disease - Why and Where It OccursdNo ratings yet
- Managing Chest DrainageDocument63 pagesManaging Chest DrainagecarlalynneNo ratings yet
- Pyogenic Spinal InfectionsDocument16 pagesPyogenic Spinal InfectionsFrancisco Escobar MoralesNo ratings yet
- LabsDocument114 pagesLabsDrSabah LotfyNo ratings yet
- Patient FinalDocument51 pagesPatient FinalCharmmaine Yu-AcmanNo ratings yet
- Incidence of Lumbosacral Radiculoplexus Neuropathy and Association with DiabetesDocument8 pagesIncidence of Lumbosacral Radiculoplexus Neuropathy and Association with DiabetesMohammad AjiNo ratings yet
- Library Thesis 2014Document66 pagesLibrary Thesis 2014Rahul Kumar MishraNo ratings yet
- DohDocument8 pagesDohJai MacanasNo ratings yet
- 770 QuestionsDocument88 pages770 Questionssmile4Dr76% (25)
- NRU HydroceleDocument7 pagesNRU HydroceleDyahFitriNo ratings yet
- Community Health Nursing Practice QuestionsDocument17 pagesCommunity Health Nursing Practice QuestionsJho MagadanNo ratings yet
- Biology of Prostate Specific Antigen PDFDocument9 pagesBiology of Prostate Specific Antigen PDFKaren BotiaNo ratings yet
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocument9 pagesDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoNo ratings yet
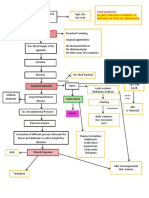
- CPC - Appendicitis (Flowchart)Document1 pageCPC - Appendicitis (Flowchart)Milet NacionalesNo ratings yet
- Causes and Effects of Restless Leg Syndrome and SunburnDocument7 pagesCauses and Effects of Restless Leg Syndrome and SunburnJacobPadillaNo ratings yet
- Breast MRI Teaching Atlas by Richard Ha, Christopher E. Comstock, Elizabeth A. Morris (Eds.)Document65 pagesBreast MRI Teaching Atlas by Richard Ha, Christopher E. Comstock, Elizabeth A. Morris (Eds.)geovanaNo ratings yet
- FertilitateaDocument569 pagesFertilitateaalex100% (2)