You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- lIVER AbscessDocument2 pageslIVER AbscessJandz MNNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- ACCN Assignment #2Document9 pagesACCN Assignment #2Jandz MNNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- ACCN Assignment #2Document9 pagesACCN Assignment #2Jandz MNNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- ACCN Assignment #2Document9 pagesACCN Assignment #2Jandz MNNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- 24 Hour Fluid MonitoringDocument2 pages24 Hour Fluid MonitoringJandz MNNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Textbook DiscussionDocument3 pagesTextbook DiscussionJandz MNNo ratings yet
- Heart DevelopmentDocument24 pagesHeart DevelopmentJandz MNNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Patient Assignment-1Document1 pagePatient Assignment-1Jandz MNNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Tof Schematic DiagramDocument3 pagesTof Schematic DiagramJandz MNNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Metronidazole generic dosage indications reactionsDocument1 pageMetronidazole generic dosage indications reactionsiluvmunicamuchNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Evaluation Sheet: Registration Process (Generally)Document1 pageEvaluation Sheet: Registration Process (Generally)Jandz MNNo ratings yet
- P Francis. Ign Feastday. For PrintDocument6 pagesP Francis. Ign Feastday. For PrintJandz MNNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Self Assessment Tool NAMSSDocument5 pagesSelf Assessment Tool NAMSSJandz MNNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Gastroenteritis GuidelineDocument15 pagesGastroenteritis GuidelineJandz MNNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Cover PageDocument1 pageCover PageJandz MNNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ReferencesDocument5 pagesReferencesJandz MNNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Table of ContentsDocument1 pageTable of ContentsJandz MNNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- World CivilizationDocument15 pagesWorld CivilizationJandz MNNo ratings yet
- ICU Case Pre - Labs DRFTDocument9 pagesICU Case Pre - Labs DRFTJandz MNNo ratings yet
- Schem DiDocument3 pagesSchem DiJandz MNNo ratings yet
- Evaluation Sheet: Registration Process (Generally)Document1 pageEvaluation Sheet: Registration Process (Generally)Jandz MNNo ratings yet
- Results Normal Values Significance Blood Gas Values Hco Tco Bevv O Sat Temporary Corrected Values Ph-Paco PaoDocument1 pageResults Normal Values Significance Blood Gas Values Hco Tco Bevv O Sat Temporary Corrected Values Ph-Paco PaoJandz MNNo ratings yet
- Management of Acute Asthma in Adults in The EmergencyDocument14 pagesManagement of Acute Asthma in Adults in The EmergencyJandz MNNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- ICU Case Pre - Labs DRFTDocument9 pagesICU Case Pre - Labs DRFTJandz MNNo ratings yet
- Schematic Diagram MyomaDocument2 pagesSchematic Diagram MyomaJandz MN100% (2)
- Sports BeatDocument34 pagesSports BeatJandz MNNo ratings yet
- Schematic Diagram Intramural MyomaDocument3 pagesSchematic Diagram Intramural MyomaJandz MNNo ratings yet
- Monopolistic CompetitionDocument29 pagesMonopolistic CompetitionJandz MNNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- TOF Schem DiDocument3 pagesTOF Schem DiJandz MNNo ratings yet
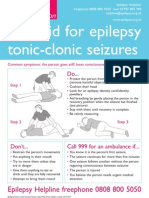
- Epilepsyaction FirstaidpostersDocument2 pagesEpilepsyaction FirstaidpostersKheliwiNo ratings yet
- Clinical Neurosurgical Vignettes For The Oral Board and Recertification Examinations First 2 Chapters PDFDocument27 pagesClinical Neurosurgical Vignettes For The Oral Board and Recertification Examinations First 2 Chapters PDFece142100% (2)
- Anatomy and Physiology of Blood VesselDocument3 pagesAnatomy and Physiology of Blood Vesselneleh grayNo ratings yet
- Neurology Notes Syrian StudentDocument5 pagesNeurology Notes Syrian StudentLiridon SopajNo ratings yet
- Tigrinya Medical LSKDocument120 pagesTigrinya Medical LSKTesfa Wele100% (1)
- Neurological AssessmentDocument64 pagesNeurological AssessmentNEuRoLoGisT CoFFeeCuP95% (20)
- Unti 4-6 StudyDocument1 pageUnti 4-6 StudyJennifer Schulze AyscueNo ratings yet
- Chiari MalformationDocument15 pagesChiari Malformationapi-388981686No ratings yet
- Doh - Mental Health Gap Action ProgramDocument4 pagesDoh - Mental Health Gap Action ProgramCassey AnneNo ratings yet
- Final Case Study JindalDocument39 pagesFinal Case Study JindalSahil SinglaNo ratings yet
- Manual de Neuropatía Periférica (2005)Document727 pagesManual de Neuropatía Periférica (2005)histoginoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Neurotransmitter ChartDocument1 pageNeurotransmitter ChartEduardo LauandeNo ratings yet
- GCSDocument76 pagesGCSJane PalafoxNo ratings yet
- 4 5866212804146498341Document36 pages4 5866212804146498341Faris FirasNo ratings yet
- Clinical Aspects of UMN LMNDocument24 pagesClinical Aspects of UMN LMNKelly YeowNo ratings yet
- Nervous System Chapter EssentialsDocument19 pagesNervous System Chapter EssentialsAeren RhosenNo ratings yet
- Certificaiton of Rachel Alintoff - RevisedDocument11 pagesCertificaiton of Rachel Alintoff - Revisedmikekvolpe100% (1)
- Frequent Headaches: Evaluation and Management: Patients WithDocument10 pagesFrequent Headaches: Evaluation and Management: Patients WithRami ElnakatNo ratings yet
- Multiple SclerosisDocument96 pagesMultiple SclerosisDrGasnasNo ratings yet
- 1 - 2 - Module 1 (Neuroanatomy) - Part 1 - Learning Objectives and Overview of Neuroanatomy (27-46)Document14 pages1 - 2 - Module 1 (Neuroanatomy) - Part 1 - Learning Objectives and Overview of Neuroanatomy (27-46)Rodrigo Eberhart Musaio SommaNo ratings yet
- Sensing the environment: Sight 視覺Document3 pagesSensing the environment: Sight 視覺Winnie ChanNo ratings yet
- Convulsion Neo Flujograma 11 NicusDocument8 pagesConvulsion Neo Flujograma 11 NicusYolanda RodriguezNo ratings yet
- Audiogram InterpretationDocument5 pagesAudiogram InterpretationSusan JackmanNo ratings yet
- III. Mcqs NeuroDocument19 pagesIII. Mcqs NeuroMhmd Iraky100% (1)
- Cns PathologyDocument18 pagesCns Pathologysunnyorange8No ratings yet
- Multiple Sclerosis Concept MapDocument1 pageMultiple Sclerosis Concept MapKyle Santos50% (2)
- Non-Convulsive Status EpilepticusDocument17 pagesNon-Convulsive Status EpilepticusjossNo ratings yet
- Dissertationen Online Uni Bonn MedizinDocument8 pagesDissertationen Online Uni Bonn MedizinHelpWithWritingAPaperUK100% (1)
- PG Prospectus 2021Document41 pagesPG Prospectus 2021Amy LalringhluaniNo ratings yet
- Electroencephalography (Eeg)Document13 pagesElectroencephalography (Eeg)Shelten GeorgeNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)