You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Engineering MaterialsDocument16 pagesEngineering MaterialsYosef Ganang Jati NugrohoNo ratings yet
- Concrete Society - Concrete Advice No 26 - RC Bund StructuresDocument3 pagesConcrete Society - Concrete Advice No 26 - RC Bund StructuresKarishma JuttunNo ratings yet
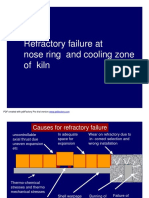
- Nose Ring & Retaining Ring - Cooling & Refractory DesignDocument69 pagesNose Ring & Retaining Ring - Cooling & Refractory Designzementhead100% (3)
- Plant CompetitionDocument4 pagesPlant CompetitionEugenTutunaruNo ratings yet
- 8 Grade Chemistry Unit Review: Name: Teacher: Date: Laylee Taghizadeh Stegemann April 19, 2021Document4 pages8 Grade Chemistry Unit Review: Name: Teacher: Date: Laylee Taghizadeh Stegemann April 19, 2021Laylee TaghizadehNo ratings yet
- Hyundai HL780-3ADocument636 pagesHyundai HL780-3AAnonymous yjK3peI740% (5)
- Extreme Taste of Faith Permission Form 2014Document1 pageExtreme Taste of Faith Permission Form 2014Corpus Christi ChurchNo ratings yet
- Corpus Christi Camp Wow 2014 Registration and Permission FormDocument3 pagesCorpus Christi Camp Wow 2014 Registration and Permission FormCorpus Christi ChurchNo ratings yet
- YLC 2014 Permission Forms.Document1 pageYLC 2014 Permission Forms.Corpus Christi ChurchNo ratings yet
- YLC Forms 2014Document1 pageYLC Forms 2014Corpus Christi ChurchNo ratings yet
- OUR LADY OF ANGELS MISSION Authorization Form: General PermissionDocument1 pageOUR LADY OF ANGELS MISSION Authorization Form: General PermissionCorpus Christi ChurchNo ratings yet
- 2013 Peer Ministry Retreat FormDocument2 pages2013 Peer Ministry Retreat FormCorpus Christi ChurchNo ratings yet
- Creed Study SeriesDocument1 pageCreed Study SeriesCorpus Christi ChurchNo ratings yet
- Mission Trip Form 2013Document1 pageMission Trip Form 2013Corpus Christi ChurchNo ratings yet
- Mission Trip Adult Med Form 2013Document1 pageMission Trip Adult Med Form 2013Corpus Christi ChurchNo ratings yet
- Youth Medical Form Mission Trip 2013Document1 pageYouth Medical Form Mission Trip 2013Corpus Christi ChurchNo ratings yet
- Confirmation FormsDocument8 pagesConfirmation FormsCorpus Christi ChurchNo ratings yet
- Colorcontin VGPDocument3 pagesColorcontin VGPasebaei95No ratings yet
- Tappi Extrution Coating and LaminatingDocument26 pagesTappi Extrution Coating and LaminatingKhương HuỳnhNo ratings yet
- Biochem Exam Practice QuestionsDocument12 pagesBiochem Exam Practice Questionsihack_101No ratings yet
- Notes For Teacher: Thin Layer Chromatography Analysis and Purification of Aspirin by RecrystallizationDocument3 pagesNotes For Teacher: Thin Layer Chromatography Analysis and Purification of Aspirin by RecrystallizationCleraNo ratings yet
- Exp 10 Alkyl HalidesDocument18 pagesExp 10 Alkyl HalidesGeorge PiliposyanNo ratings yet
- Nato - Stanag 4582 - Explosives, Nitrocellulose Based Propellants, Stability Test Procedure and Requirements Using Heat Flow CalorimetryDocument25 pagesNato - Stanag 4582 - Explosives, Nitrocellulose Based Propellants, Stability Test Procedure and Requirements Using Heat Flow CalorimetryTetis BrionesNo ratings yet
- Foundry Workshop ManualDocument22 pagesFoundry Workshop Manuallakshya100% (1)
- Chemical Engineering Board Exam PDFDocument3 pagesChemical Engineering Board Exam PDFJohn Leonard FazNo ratings yet
- Chemical MachiningDocument5 pagesChemical MachiningomenNo ratings yet
- Export Product Hand BookDocument94 pagesExport Product Hand Bookamit singhNo ratings yet
- Topic 1 - Stoichiometric Relationships - Part 1 - AnswersDocument26 pagesTopic 1 - Stoichiometric Relationships - Part 1 - Answersburcak gecNo ratings yet
- 0620 m23 QP 22-MinDocument14 pages0620 m23 QP 22-Minjelani17fNo ratings yet
- Titration Strong Weak Acids BasesDocument6 pagesTitration Strong Weak Acids Basesapi-309713761No ratings yet
- Bell & Gosset PumpDocument8 pagesBell & Gosset Pumprogel_ganaNo ratings yet
- Emkarate RL 32H: Material Safety Data Sheet Date Revised: Feb, 2008Document6 pagesEmkarate RL 32H: Material Safety Data Sheet Date Revised: Feb, 2008angelo collaNo ratings yet
- Certificate: Internal Teacher's SignDocument8 pagesCertificate: Internal Teacher's SignVyomNo ratings yet
- Pricelist Juli 2023 UserDocument108 pagesPricelist Juli 2023 Userfitri heriyati pratiwiNo ratings yet
- Jack WelchDocument5 pagesJack Welchapi-314805892No ratings yet
- HSC Chemistry Lesson Plan 19Document5 pagesHSC Chemistry Lesson Plan 19Ali HaidarNo ratings yet
- 5meo SynthesisDocument2 pages5meo SynthesisLuis López PiñeresNo ratings yet
- Basics of SMAWDocument157 pagesBasics of SMAWAsad Bin Ala QatariNo ratings yet
- A Detailed Lesson Plan in Health Grade 8 - 1 Quarter A. Content StandardDocument6 pagesA Detailed Lesson Plan in Health Grade 8 - 1 Quarter A. Content StandardIsmael Jefferson De AsisNo ratings yet
- TSADocument44 pagesTSAdraj1875977No ratings yet
- Bacterial ConjugationDocument5 pagesBacterial ConjugationPrasenjit VighneNo ratings yet