You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Viral DiseasesDocument35 pagesViral DiseasesDivya SoundarajanNo ratings yet
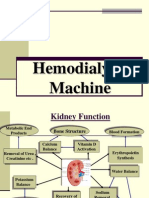
- Hemodialysis Machine12Document45 pagesHemodialysis Machine12Divya SoundarajanNo ratings yet
- ECE 301 - Digital Electronics: Flip-Flops and RegistersDocument36 pagesECE 301 - Digital Electronics: Flip-Flops and RegistersDivya SoundarajanNo ratings yet
- Someone You Know Has MS: A Book For FamiliesDocument19 pagesSomeone You Know Has MS: A Book For FamiliesDivya SoundarajanNo ratings yet
- Addressing Modes of 8085Document10 pagesAddressing Modes of 8085etfs4indiaNo ratings yet
- BmiDocument3 pagesBmiDivya SoundarajanNo ratings yet
- Mathematics 1 QB - PART - ADocument6 pagesMathematics 1 QB - PART - ADivya SoundarajanNo ratings yet
- Datis KharrazianDocument25 pagesDatis Kharraziangreym111100% (1)
- HashimotoDocument9 pagesHashimotoFrinkooFrinkoBNo ratings yet
- Vanderlugt 2002Document11 pagesVanderlugt 2002Hashem Essa QatawnehNo ratings yet
- Urticaria: Collegium Internationale Allergologicum (CIA) Update 2020Document13 pagesUrticaria: Collegium Internationale Allergologicum (CIA) Update 2020Ihdinal MuktiNo ratings yet
- The Lymphatic System and Body Defenses: Part BDocument67 pagesThe Lymphatic System and Body Defenses: Part BJovelle AlcantaraNo ratings yet
- Immunotolerance and Autoimmune DiseasesDocument37 pagesImmunotolerance and Autoimmune DiseasesmulatumeleseNo ratings yet
- Autoimmunity and DisordersDocument54 pagesAutoimmunity and DisordersInjamam ul hossainNo ratings yet
- CK-12 Biology Chapter 24 WorksheetsDocument32 pagesCK-12 Biology Chapter 24 WorksheetsShermerNo ratings yet
- Warm Autoimmune Hemolytic Anemia: Advances in Pathophysiology and TreatmentDocument8 pagesWarm Autoimmune Hemolytic Anemia: Advances in Pathophysiology and TreatmentMishel PazmiñoNo ratings yet
- PD2Document15 pagesPD2DrShobhit RajNo ratings yet
- SerologyDocument33 pagesSerologyGEBEYAW ADDISUNo ratings yet
- Pathophysiology Examination AnswersDocument205 pagesPathophysiology Examination AnswersFırat Güllü67% (6)
- International Journal of Immunology and Immunotherapy Ijii 9 064Document5 pagesInternational Journal of Immunology and Immunotherapy Ijii 9 064jongsu kimNo ratings yet
- Epidemiology and Clinical Features of Multiple Sclerosis in Adults Uptodate3Document11 pagesEpidemiology and Clinical Features of Multiple Sclerosis in Adults Uptodate3Régulo RafaelNo ratings yet
- Medical AbbreviationDocument76 pagesMedical AbbreviationNajwa AbdullahNo ratings yet
- Autoimmune DiseasesDocument26 pagesAutoimmune DiseasesCherry Reyes-PrincipeNo ratings yet
- Microbiology: A Systems Approach, 2 Ed.: Chapter 16: Disorders in ImmunityDocument76 pagesMicrobiology: A Systems Approach, 2 Ed.: Chapter 16: Disorders in ImmunityJes OngNo ratings yet
- Specific and Non Specific Immmune System: DR Nova Kurniati, Sppd. K-Ai. FinasimDocument88 pagesSpecific and Non Specific Immmune System: DR Nova Kurniati, Sppd. K-Ai. FinasimamaliakhaNo ratings yet
- A Doctor's 4-Step Program To Treat Autoimmune Disease: THE IMMUNE SYSTEM RECOVERY PLAN by Susan BlumDocument65 pagesA Doctor's 4-Step Program To Treat Autoimmune Disease: THE IMMUNE SYSTEM RECOVERY PLAN by Susan BlumSimon and Schuster85% (26)
- Gel Formulation of Drug X Drug and Evaluate Its EfficacyDocument26 pagesGel Formulation of Drug X Drug and Evaluate Its EfficacyPriyanka YadavNo ratings yet
- Carbohydrate Metabolism Disorders Stom 10-11Document61 pagesCarbohydrate Metabolism Disorders Stom 10-11Artem GrigoryanNo ratings yet
- Anti-Inflammatory Injectable SolutionDocument6 pagesAnti-Inflammatory Injectable SolutionminunatNo ratings yet
- Topic 5 - Handbook of Medical Sociology Ch4 - 2Document23 pagesTopic 5 - Handbook of Medical Sociology Ch4 - 2AngellaNo ratings yet
- Rachmat Gunadi Wachjudi's resume and clinical relevance of vitamin DDocument38 pagesRachmat Gunadi Wachjudi's resume and clinical relevance of vitamin DNururrohmahNo ratings yet
- Eponyms SyndromesDocument23 pagesEponyms Syndromestekennn021No ratings yet
- Hemolytic AnemiaDocument1 pageHemolytic AnemiaTeus FatamorganaNo ratings yet
- Diagnosis and Management of Paediatric Autoimmune Hepatitis AIH. ESPGHAN Advice Guide. 2019. Ver1.Document4 pagesDiagnosis and Management of Paediatric Autoimmune Hepatitis AIH. ESPGHAN Advice Guide. 2019. Ver1.Carmen OpreaNo ratings yet
- Th1 - Th2 Dominance SymptomsListDocument3 pagesTh1 - Th2 Dominance SymptomsListikuus123No ratings yet
- Diabetes Ebook:Type 1 Diabetes in AdultsDocument88 pagesDiabetes Ebook:Type 1 Diabetes in AdultsHealthCare0% (1)
- Immunotoxicology EvaluationDocument38 pagesImmunotoxicology EvaluationVlad TomaNo ratings yet