You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- W SW 2Document192 pagesW SW 2gjuiolpNo ratings yet
- W SW 2Document192 pagesW SW 2gjuiolpNo ratings yet
- Height Increase JournalDocument63 pagesHeight Increase JournalgjuiolpNo ratings yet
- GTA CodeDocument5 pagesGTA CodegjuiolpNo ratings yet
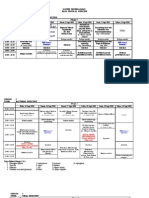
- Jadwal TROPMED 10Document6 pagesJadwal TROPMED 10Ryan HendryNo ratings yet
- Seminar Ketahanan Pangan Sapi Perah 2Document10 pagesSeminar Ketahanan Pangan Sapi Perah 2gjuiolpNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Thesis 97Document109 pagesThesis 97shahzadanjum333100% (1)
- Transient Ischemic Attacks: Rodney W. Smith, MDDocument58 pagesTransient Ischemic Attacks: Rodney W. Smith, MDNatalija TomićNo ratings yet
- Vestibular Neuritis HandoutDocument3 pagesVestibular Neuritis HandoutPrisilia QurratuAiniNo ratings yet
- The Efficacy of Venlafaxine, Flunarizine, and Valproic Acid in The Prophylaxis of Vestibular MigraineDocument5 pagesThe Efficacy of Venlafaxine, Flunarizine, and Valproic Acid in The Prophylaxis of Vestibular MigraineagustianaNo ratings yet
- Primary Care Guidelines VertigoDocument1 pagePrimary Care Guidelines VertigoSyahidatul Kautsar NajibNo ratings yet
- Central VertigoDocument9 pagesCentral VertigoDiayanti TentiNo ratings yet
- Soap Notes 101Document45 pagesSoap Notes 101CELINE MARTJOHNSNo ratings yet
- ENT CourseDocument29 pagesENT Coursetaliya. shvetzNo ratings yet
- Journal of Clinical Gerontology & Geriatrics: Pradnya Dhargave, PHD, Ragupathy Sendhilkumar, MSC, MPTDocument5 pagesJournal of Clinical Gerontology & Geriatrics: Pradnya Dhargave, PHD, Ragupathy Sendhilkumar, MSC, MPTAlfianGafarNo ratings yet
- The Body MeridiansDocument61 pagesThe Body MeridiansAnonymous NKGMQv9100% (9)
- اسئلة neuroDocument30 pagesاسئلة neuroSoad RedaNo ratings yet
- Analysis of Persistent Geotropic and Apogeotropic Positional Nystagmus of The Lateral Canal Benign Paroxysmal Positional VertigoDocument6 pagesAnalysis of Persistent Geotropic and Apogeotropic Positional Nystagmus of The Lateral Canal Benign Paroxysmal Positional VertigoRudolfGerNo ratings yet
- Course 3 - Trauamt UrechiiDocument13 pagesCourse 3 - Trauamt UrechiiLiviu LivaxNo ratings yet
- Dizziness and VertigoDocument27 pagesDizziness and VertigoPutriAyuWidyastutiRNo ratings yet
- MeniereDocument5 pagesMeniereMayls Sevilla CalizoNo ratings yet
- Vertiginous EpilepsyDocument5 pagesVertiginous Epilepsyzudan2013No ratings yet
- AnatoFisio VestibularDocument17 pagesAnatoFisio VestibularRocío YáñezNo ratings yet
- Article 1519801601Document4 pagesArticle 1519801601Graziela SpadariNo ratings yet
- ENT Notes CrakDocument52 pagesENT Notes CrakGrant KimNo ratings yet
- Clinical Practice Guideline - Ménière's Disease PDFDocument56 pagesClinical Practice Guideline - Ménière's Disease PDFCarol Natalia Fonseca SalgadoNo ratings yet
- Nausea and Vomiting in Adolescents and AdultsDocument30 pagesNausea and Vomiting in Adolescents and AdultsPramita Ines ParmawatiNo ratings yet
- Finals Reviewer and Activities NCM 116 LecDocument24 pagesFinals Reviewer and Activities NCM 116 LecMary CruzNo ratings yet
- Talley & O'Connor Quiz SampleDocument5 pagesTalley & O'Connor Quiz SamplefilchibuffNo ratings yet
- 2011-Visual Analog Scale To Assess Vertigo and Dizziness After Repositioning Maneuvers For Benign Paroxysmal Positional VertigoDocument7 pages2011-Visual Analog Scale To Assess Vertigo and Dizziness After Repositioning Maneuvers For Benign Paroxysmal Positional VertigoPingShun ChenNo ratings yet
- Cerebellar InfarctionDocument23 pagesCerebellar InfarctionShane LuyNo ratings yet
- Family Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesDocument6 pagesFamily Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesAndrea Kristin OrigenesNo ratings yet
- The Positive Times Newspaper - Wadsworth June 2011Document20 pagesThe Positive Times Newspaper - Wadsworth June 2011positivetimesNo ratings yet
- Neurologic Disorders - NCM 102 LecturesDocument12 pagesNeurologic Disorders - NCM 102 LecturesBernard100% (4)
- ENT AyaSalahEldeenDocument147 pagesENT AyaSalahEldeenFatma ShnewraNo ratings yet
- Otorrino ContinuumDocument220 pagesOtorrino ContinuumRafaelNo ratings yet