You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Engleza Intensiv - Subiectul I - Variante 001-100 - An 2008Document171 pagesEngleza Intensiv - Subiectul I - Variante 001-100 - An 2008Admin100% (4)
- HTM 02-01 Part BDocument162 pagesHTM 02-01 Part Bloirees100% (1)
- Toate Subiectele Sunt Obligatorii. Se Acord Timpul Efectiv de Lucru Este de 3 OreDocument2 pagesToate Subiectele Sunt Obligatorii. Se Acord Timpul Efectiv de Lucru Este de 3 OreloireesNo ratings yet
- Gramatica Limbii Engleze Prin Idiomuri - Cristina IonescuDocument79 pagesGramatica Limbii Engleze Prin Idiomuri - Cristina IonesculoireesNo ratings yet
- Medical Devices - Guidance DocumentDocument22 pagesMedical Devices - Guidance DocumentloireesNo ratings yet
- Quick Activities To Build A Very Voluminous Vocabulary GR 4-8Document64 pagesQuick Activities To Build A Very Voluminous Vocabulary GR 4-8loirees75% (4)
- (WWW - Fisierulmeu.ro) Round-Up 3 PDFDocument163 pages(WWW - Fisierulmeu.ro) Round-Up 3 PDFilincabarbie100% (1)
- Penguin Readers Level 4 King Solomons MinesDocument20 pagesPenguin Readers Level 4 King Solomons Minesloirees100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Human Anatomy,: First Edition Mckinley & O'LoughlinDocument65 pagesHuman Anatomy,: First Edition Mckinley & O'Loughlinİsmail ŞimşekNo ratings yet
- Medical Emergencies in Dental Practice A Nationwide Web-BasedDocument12 pagesMedical Emergencies in Dental Practice A Nationwide Web-BasedVidyandika PermanasariNo ratings yet
- Uso de Albúmina en CirrosisDocument12 pagesUso de Albúmina en CirrosisSMIBA MedicinaNo ratings yet
- Aurum MetallicumDocument6 pagesAurum MetallicumSuhas IngaleNo ratings yet
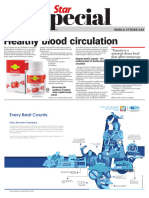
- World Stroke Day - 29 October 2023Document5 pagesWorld Stroke Day - 29 October 2023Times MediaNo ratings yet
- Grand Case PresentationDocument50 pagesGrand Case PresentationJean Michelle100% (1)
- Dyslipidemia - From Prevention To TreatmentDocument480 pagesDyslipidemia - From Prevention To Treatmentsyahputra88100% (1)
- Renal FailureDocument27 pagesRenal FailureMae DacerNo ratings yet
- FinalDocument36 pagesFinalNirali GalaNo ratings yet
- Hot Topics in Heart Failure: New Data and Therapies That Are Changing The Treatment LandscapeDocument70 pagesHot Topics in Heart Failure: New Data and Therapies That Are Changing The Treatment LandscapeSasmita DewiNo ratings yet
- Animal Circulation and RespirationDocument56 pagesAnimal Circulation and Respirationacooper6No ratings yet
- 2016 4. Clin Med Reviewer NeuroSpine Abdomen Pages 1 734 5576 90 P44.00Document90 pages2016 4. Clin Med Reviewer NeuroSpine Abdomen Pages 1 734 5576 90 P44.00Patricia HariramaniNo ratings yet
- NCMB 312 Lec Course Task CU2: Our Lady of Fatima UniversityDocument2 pagesNCMB 312 Lec Course Task CU2: Our Lady of Fatima UniversityMushy_ayaNo ratings yet
- Abduraham Rayyan-Module-Cardiovascular-SystemDocument17 pagesAbduraham Rayyan-Module-Cardiovascular-SystemRAYYAN ENIL ABDURAHAMNo ratings yet
- STEP 2 CK New Free 120 (Q)Document59 pagesSTEP 2 CK New Free 120 (Q)M. Baidar SaeedNo ratings yet
- Case Study With ECG Reading OcañaDocument3 pagesCase Study With ECG Reading OcañaNicole Chloe OcanaNo ratings yet
- E Cigarettes Policy BriefDocument16 pagesE Cigarettes Policy Brieftht 21No ratings yet
- Urinary System LecDocument7 pagesUrinary System LecMax DelvalleNo ratings yet
- Post Guidelines - June 16Document52 pagesPost Guidelines - June 16kevin clone1No ratings yet
- Albumin Blood Kidneys Kidneys KidneysDocument1 pageAlbumin Blood Kidneys Kidneys Kidneysjamal khanNo ratings yet
- Anatomy Slides 2019-08-21 ALLDocument59 pagesAnatomy Slides 2019-08-21 ALLMonica MoyaNo ratings yet
- Musallam 2018Document7 pagesMusallam 2018Koup NuNo ratings yet
- Ebook Goldbergers Clinical Electrocardiography A Simplified Approach PDF Full Chapter PDFDocument52 pagesEbook Goldbergers Clinical Electrocardiography A Simplified Approach PDF Full Chapter PDFjames.farnan170100% (23)
- 6 HypertensionDocument5 pages6 Hypertensionجنى الجنان عقد الجمانNo ratings yet
- Common Complications of Iv TherapyDocument63 pagesCommon Complications of Iv TherapyFrancis James RigodonNo ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- BLS Module Final AHA - Revised May 21-2012Document194 pagesBLS Module Final AHA - Revised May 21-2012meljamerlan100% (4)
- Chapter 5 ExercisesDocument10 pagesChapter 5 Exercisesshafilcr07No ratings yet
- Step by Step EchocardiographyDocument141 pagesStep by Step EchocardiographyMonica Surdu83% (6)
- Pathophysiology & Concept Map: Precipitating FactorsDocument2 pagesPathophysiology & Concept Map: Precipitating FactorsVanessa Rose Vargas0% (1)