You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- API 570 Piping InspectionDocument35 pagesAPI 570 Piping InspectionIrvansyah Razadin100% (9)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Box Culvert Limit StateDocument52 pagesBox Culvert Limit StateMahadev Sastry88% (8)
- CH 06Document79 pagesCH 06arif nugraha67% (3)
- Parts Manual Keeway Fact 50 2tDocument61 pagesParts Manual Keeway Fact 50 2tSimon Albert100% (1)
- Haryana Exporters Complete ListDocument8 pagesHaryana Exporters Complete ListShashank SrivastavaNo ratings yet
- 571.302 Standard No. 302 Flammability of Interior MaterialsDocument3 pages571.302 Standard No. 302 Flammability of Interior MaterialsTomáš Ryba100% (1)
- Rollingstock Operations MatrixDocument1 pageRollingstock Operations MatrixyrperdanaNo ratings yet
- Philippine Highway ActDocument15 pagesPhilippine Highway ActJordan TumayanNo ratings yet
- S AA GEN CDF (Civ Design Fundamental) (Rev.0 2009)Document17 pagesS AA GEN CDF (Civ Design Fundamental) (Rev.0 2009)Mohammad Al JedyNo ratings yet
- Project Ideas PDDocument56 pagesProject Ideas PDrobiromasNo ratings yet
- Amsa 1566Document6 pagesAmsa 1566TrucMaiNo ratings yet
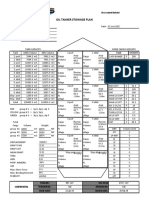
- Group 4 RDF 027 Oil Tanker Stowage Plan Rev 1.0 EditableDocument1 pageGroup 4 RDF 027 Oil Tanker Stowage Plan Rev 1.0 Editablegidjuns abs100% (1)
- Egjj/Jer Jersey, Uk: Gur Vor DmeDocument27 pagesEgjj/Jer Jersey, Uk: Gur Vor DmeTweed3ANo ratings yet
- Chapter 14 Post Construction Jan2013Document37 pagesChapter 14 Post Construction Jan2013Asim Amin100% (1)
- Fe42rl GBR EngDocument4 pagesFe42rl GBR EngaaNo ratings yet
- Practice Problems 14: Influence LineDocument8 pagesPractice Problems 14: Influence LineMikhael Wakin RodriguezNo ratings yet
- Country Report On Building Energy Codes in Japan: M Evans B Shui T TakagiDocument31 pagesCountry Report On Building Energy Codes in Japan: M Evans B Shui T Takagibcap-oceanNo ratings yet
- Lifting PlatformsDocument12 pagesLifting PlatformsHector MoragaNo ratings yet
- Q 117R2Document2 pagesQ 117R22791957No ratings yet
- Prague - HotelsDocument34 pagesPrague - HotelsKodro JohnNo ratings yet
- Vw-Wi RL V.en-GB.K00589703.wi 47742071 PDFDocument2 pagesVw-Wi RL V.en-GB.K00589703.wi 47742071 PDFAndreas AndreouNo ratings yet
- SubwaymapnyDocument1 pageSubwaymapnyMilica TodorovicNo ratings yet
- CS / GI To PE Fittings (I.e. Transition Fittings of Sizes 20 MM To 63 MM)Document4 pagesCS / GI To PE Fittings (I.e. Transition Fittings of Sizes 20 MM To 63 MM)Raman KumarNo ratings yet
- Adika - Final - Thesis - April 28 With Additional Edits From WasDocument60 pagesAdika - Final - Thesis - April 28 With Additional Edits From WasAdikaM.RahimliNo ratings yet
- 285 PSV Seacor WarriorDocument2 pages285 PSV Seacor WarriorNayo Sanchez CrespoNo ratings yet
- 1 - FplanEDDMEDDHDocument32 pages1 - FplanEDDMEDDHzackNo ratings yet
- Ashish Jha (Cop)Document1 pageAshish Jha (Cop)ashishjha6067No ratings yet
- Cargo Carrier Owner'S Manual: Item #142479Document8 pagesCargo Carrier Owner'S Manual: Item #142479kopljanikNo ratings yet
- Crown SP 3500 Stock Picker Lift Truck Operator's Manual PDFDocument22 pagesCrown SP 3500 Stock Picker Lift Truck Operator's Manual PDFVüsal 1No ratings yet
- Vehicles Inspection Check List: Karros Show Import S.C.R.L 346-0982 99827 7201 99827 3318 99408 8106Document6 pagesVehicles Inspection Check List: Karros Show Import S.C.R.L 346-0982 99827 7201 99827 3318 99408 8106jorgedavid31No ratings yet