You might also like
- Health Assessment in Nursing 7th Edition by Weber KelleyDocument261 pagesHealth Assessment in Nursing 7th Edition by Weber KelleyMouad Faouzi100% (7)
- Surg Wound Clas TreeDocument1 pageSurg Wound Clas TreeCita Rahma SwastikaNo ratings yet
- Rehabilitation of Patients Suffering Trigeminal Nerve NeuragiaDocument22 pagesRehabilitation of Patients Suffering Trigeminal Nerve NeuragiacosornoNo ratings yet
- Neurological Disturbances of FaceDocument33 pagesNeurological Disturbances of FaceDrMuskan AroraNo ratings yet
- Management of NeuralgiaDocument2 pagesManagement of NeuralgiaNeivashini MaDhavanNo ratings yet
- Trigeminal NeurlgiaDocument5 pagesTrigeminal NeurlgiaAnonymous V1tCwPHlDNo ratings yet
- What Is Trigeminal NeuralgiaDocument3 pagesWhat Is Trigeminal NeuralgiakewpietheresaNo ratings yet
- Trigeminal Neuralgia Outline ScriptDocument4 pagesTrigeminal Neuralgia Outline ScriptRogerQuxNo ratings yet
- Trigeminal Neuralgi (Kuliah)Document26 pagesTrigeminal Neuralgi (Kuliah)shofyan_2005_yarsiNo ratings yet
- Trigeminal NeuralgiaDocument15 pagesTrigeminal NeuralgiaMihir Patel75% (4)
- Trigeminal NeuralgiaDocument7 pagesTrigeminal NeuralgiaEricsonMitraNo ratings yet
- Trigeminal Neuralgia: Dr. Deepthi AthuluruDocument69 pagesTrigeminal Neuralgia: Dr. Deepthi AthuluruLakshya NainNo ratings yet
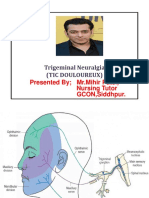
- Trigeminal Neuralgia (Tic Douloureux) : Presented by MR - Mihir Patel, Nursing Tutor GCON, SiddhpurDocument15 pagesTrigeminal Neuralgia (Tic Douloureux) : Presented by MR - Mihir Patel, Nursing Tutor GCON, Siddhpurandreas kevinNo ratings yet
- Pathophysiology, Causes, and Differential Diagnosis: Multiple SclerosisDocument4 pagesPathophysiology, Causes, and Differential Diagnosis: Multiple SclerosisjaideepbaggaNo ratings yet
- Neuralgia TrigeminalDocument5 pagesNeuralgia TrigeminalcantikarevieraNo ratings yet
- Trigeminal Neuralgia Oral SurgeryDocument48 pagesTrigeminal Neuralgia Oral SurgeryFourthMolar.com67% (3)
- NerualgiaDocument7 pagesNerualgiaKabirNo ratings yet
- Management Trigeminal NeuralgiaDocument28 pagesManagement Trigeminal NeuralgiaApeksha JadhavNo ratings yet
- Trigeminal NeuralgiaDocument5 pagesTrigeminal Neuralgiawidad syairoziNo ratings yet
- Fact Sheet Trigeminal NeuralgiaDocument2 pagesFact Sheet Trigeminal Neuralgiasarmad78No ratings yet
- Trigeminal Neuralgia (Tic Douloureux)Document49 pagesTrigeminal Neuralgia (Tic Douloureux)Mohsin HabibNo ratings yet
- Orofacial PainDocument40 pagesOrofacial Painghazy100% (1)
- What Is Trigeminal Neuralgia?Document4 pagesWhat Is Trigeminal Neuralgia?Tiger_2011No ratings yet
- Trigeminal NeuralgiaDocument54 pagesTrigeminal NeuralgiaSarah Khan100% (1)
- Neural Prolotherapy For NeuralgiaDocument4 pagesNeural Prolotherapy For NeuralgiaMariel Yarrod100% (1)
- Meningioma Brain TumorDocument5 pagesMeningioma Brain TumorNikko Melencion100% (1)
- Combat Injury OperationsDocument19 pagesCombat Injury OperationsReza ManefoNo ratings yet
- Atow 480 00Document8 pagesAtow 480 00ArhanNo ratings yet
- Craniotomy: Jump To Navigation Jump To SearchDocument6 pagesCraniotomy: Jump To Navigation Jump To SearchsakuraleeshaoranNo ratings yet
- Acc 61 - Supp2 96Document7 pagesAcc 61 - Supp2 96intermediosamberesNo ratings yet
- Facial Nerve HGGDFDocument20 pagesFacial Nerve HGGDFMaliha TahirNo ratings yet
- Trigeminal Neuralgia (Facial Pain)Document6 pagesTrigeminal Neuralgia (Facial Pain)Aisyah AlviNo ratings yet
- 15.trigeminal NeuralgiaDocument25 pages15.trigeminal NeuralgiaBhakti WashilkarNo ratings yet
- Interventional Pain ManagementDocument2 pagesInterventional Pain ManagementjosephNo ratings yet
- Wilhour-Nahas2018 Article The NeuralgiasDocument8 pagesWilhour-Nahas2018 Article The NeuralgiasCamilo Benavides BurbanoNo ratings yet
- TN OverviewDocument6 pagesTN OverviewNursing DepartmentNo ratings yet
- Inferior Alveolar Nerve Injury in Implant Dentistry: Diagnosis, Causes, Prevention, and ManagementDocument7 pagesInferior Alveolar Nerve Injury in Implant Dentistry: Diagnosis, Causes, Prevention, and ManagementmaxNo ratings yet
- Trigeminal Neuralgia 2Document48 pagesTrigeminal Neuralgia 2mszlazak4179No ratings yet
- A Case of Occipital NeuralgiaDocument20 pagesA Case of Occipital NeuralgiaLakNo ratings yet
- Varicose Vein Treatment Tips and Trick - Ablation or GlueDocument30 pagesVaricose Vein Treatment Tips and Trick - Ablation or GlueNata NakamuraNo ratings yet
- Trigeminal Neuralgia: D. LeclercqDocument9 pagesTrigeminal Neuralgia: D. LeclercqHossam ThabetNo ratings yet
- Nerve Injuries Associated With Gynecological SurgeryDocument8 pagesNerve Injuries Associated With Gynecological SurgeryLakshmi DheviNo ratings yet
- Xia 2014Document5 pagesXia 2014Akmal Niam FirdausiNo ratings yet
- Types of Operations On NervesDocument1 pageTypes of Operations On Nervesawais mpNo ratings yet
- Nervous SystemDocument29 pagesNervous SystemMuhammed Aslam NVNo ratings yet
- TrigeminalNeuralgiaPracticeEssentials, Background, Anatomy 1700148132569Document9 pagesTrigeminalNeuralgiaPracticeEssentials, Background, Anatomy 1700148132569esthersilingi12No ratings yet
- Acoustic NeuromaDocument2 pagesAcoustic NeuromaSNo ratings yet
- Lumbar Disc Disease 3Document2 pagesLumbar Disc Disease 3mohamedwhateverNo ratings yet
- Peripheral Neurectomies: A Treatment Option For Trigeminal Neuralgia in Rural PracticeDocument9 pagesPeripheral Neurectomies: A Treatment Option For Trigeminal Neuralgia in Rural PracticeMustaqim PrasetyaNo ratings yet
- Trigeminal NeuralgiaDocument18 pagesTrigeminal NeuralgiaKaran KohliNo ratings yet
- Mendoza Outline of DiseasesDocument28 pagesMendoza Outline of DiseasesAleks MendozaNo ratings yet
- Correction of The Soft Tissue Pollybeak Using Triamcinolone InjectionDocument5 pagesCorrection of The Soft Tissue Pollybeak Using Triamcinolone Injectionmiglena-filipova-5062No ratings yet
- Presented by Cathrine Diana PGI Dept of Oral and Maxillofacial SurgeryDocument78 pagesPresented by Cathrine Diana PGI Dept of Oral and Maxillofacial SurgeryDorin PathakNo ratings yet
- Anesthesia For Opthalmological SurgeriesDocument69 pagesAnesthesia For Opthalmological SurgeriesRajesh MunigialNo ratings yet
- Chapter 10 - Trigeminal NeuralgiaDocument5 pagesChapter 10 - Trigeminal NeuralgiaMuhammad IkbarNo ratings yet
- Management of Trigeminal Neuralgia. A Comparison of Two TechniquesDocument20 pagesManagement of Trigeminal Neuralgia. A Comparison of Two TechniquesAbhikNo ratings yet
- Trigeminal Neuralgia: DR Tay Kwang Hui Dept of Anaesthesia 08 January 2011Document40 pagesTrigeminal Neuralgia: DR Tay Kwang Hui Dept of Anaesthesia 08 January 2011Shalim BagusNo ratings yet
- Ultrasound (2) Edit2Document53 pagesUltrasound (2) Edit2RahmanandhikaNo ratings yet
- Microvascular Decompression For Trigeminal Neuralgia: Technical Refinement For Complication AvoidanceDocument6 pagesMicrovascular Decompression For Trigeminal Neuralgia: Technical Refinement For Complication AvoidancefespositoNo ratings yet
- Retrosigmoid Approach For Giant Cystic VestibularDocument3 pagesRetrosigmoid Approach For Giant Cystic VestibularTimothy CaldwellNo ratings yet
- Intralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?From EverandIntralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?No ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- Care Plan 1 Complex HealthDocument5 pagesCare Plan 1 Complex HealthMadison OrgillNo ratings yet
- Surgical Techs Little Black BookDocument18 pagesSurgical Techs Little Black BookMichael Lester100% (5)
- BÀI HỌCDocument13 pagesBÀI HỌCMinh Chau HoangNo ratings yet
- Case Presentation TofDocument32 pagesCase Presentation TofISLAMIC KNOWLEDGE BASED ON TRULY HADIS100% (2)
- Major & Minor Surgical Instrument: ScalpelDocument7 pagesMajor & Minor Surgical Instrument: Scalpeledgar malupengNo ratings yet
- Patient Guide To Acl Injuries: What Is The Anterior Cruciate Ligament (ACL) ?Document8 pagesPatient Guide To Acl Injuries: What Is The Anterior Cruciate Ligament (ACL) ?Subbu MNo ratings yet
- Greenslopes FacilitiesDocument3 pagesGreenslopes FacilitiesCosy NamaleNo ratings yet
- Delayed Surgical RecoveryDocument10 pagesDelayed Surgical Recoveryapi-283151124No ratings yet
- Makalah Bahasa Inggris NewDocument25 pagesMakalah Bahasa Inggris Newmei diana sara'isNo ratings yet
- How To Start When You'Re Stuck: Jason and Jodi WomackDocument17 pagesHow To Start When You'Re Stuck: Jason and Jodi WomackАлександр ЛевинNo ratings yet
- MastoidectomyDocument7 pagesMastoidectomyFrancis Arman Cabanlit0% (1)
- Philippine Consensus Statements On The Management of Non-Variceal Upper Gastrointestinal Bleeding 2012Document13 pagesPhilippine Consensus Statements On The Management of Non-Variceal Upper Gastrointestinal Bleeding 2012Danica Nicole Seco Gabon100% (1)
- DR Fabio RossiDocument3 pagesDR Fabio RossiMohsin Habib100% (1)
- Comparative Health Information Management 4th Edition Peden Solutions ManualDocument23 pagesComparative Health Information Management 4th Edition Peden Solutions Manualunworth.apnoeawldza100% (32)
- 03.04 - Intraventricular TumoursDocument185 pages03.04 - Intraventricular TumoursBivolaru AlinNo ratings yet
- Case StudyDocument11 pagesCase StudyJoan BaquiranNo ratings yet
- Outcomes of Colorectal Surgery CRS at Department of Surgical Gastroenterology Max Hospital Saket InteDocument3 pagesOutcomes of Colorectal Surgery CRS at Department of Surgical Gastroenterology Max Hospital Saket InteGI Cancer IndiaNo ratings yet
- Ehs Hospitals All StatesDocument85 pagesEhs Hospitals All Statesnaiduu497No ratings yet
- Agm 2016 Businress Responbility Report 2016 PDFDocument19 pagesAgm 2016 Businress Responbility Report 2016 PDFShayant PathakNo ratings yet
- CGHS Mumbai 2010 Rate List Updated On 29th June 2021Document45 pagesCGHS Mumbai 2010 Rate List Updated On 29th June 2021nishu solankiNo ratings yet
- Anesth Essays ResDocument8 pagesAnesth Essays ResFi NoNo ratings yet
- Shouldice HospitalDocument27 pagesShouldice Hospitalredkarravina100% (1)
- Inspection Frequencies ECRIDocument2 pagesInspection Frequencies ECRIJose Arias100% (1)
- Industry 4.0 in Healthcare IndustryDocument10 pagesIndustry 4.0 in Healthcare IndustryAnand BhagwaniNo ratings yet
- Minimum Standard Requirements For 100 AdmissionsDocument88 pagesMinimum Standard Requirements For 100 AdmissionsKirthinath BallalNo ratings yet
- Midface Fractures PART IIDocument64 pagesMidface Fractures PART IIJomi Porinchu100% (1)
- Post Op InstructionsDocument12 pagesPost Op Instructionssammyjo12No ratings yet
- YasargilDocument623 pagesYasargilRicardo SantosNo ratings yet