You might also like
- Orofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsDocument49 pagesOrofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsmishaNo ratings yet
- Trigeminal Neuralgia Oral SurgeryDocument48 pagesTrigeminal Neuralgia Oral SurgeryFourthMolar.com67% (3)
- Trigeminal Neuralgia (Tic Douloureux)Document49 pagesTrigeminal Neuralgia (Tic Douloureux)Mohsin HabibNo ratings yet
- Mendoza Outline of DiseasesDocument28 pagesMendoza Outline of DiseasesAleks MendozaNo ratings yet
- Trigeminal Neuralgia: Dr. Deepthi AthuluruDocument69 pagesTrigeminal Neuralgia: Dr. Deepthi AthuluruLakshya NainNo ratings yet
- What Is Trigeminal Neuralgia?Document4 pagesWhat Is Trigeminal Neuralgia?Tiger_2011No ratings yet
- Trigeminal NeuralgiaDocument3 pagesTrigeminal NeuralgiaAira Alaro50% (2)
- Rehabilitation of Patients Suffering Trigeminal Nerve NeuragiaDocument22 pagesRehabilitation of Patients Suffering Trigeminal Nerve NeuragiacosornoNo ratings yet
- Trigeminal Neuralgia: Rowena R. Tosoc RN, PHDDocument54 pagesTrigeminal Neuralgia: Rowena R. Tosoc RN, PHDMARICRIS NEBIARNo ratings yet
- Trigeminal Neuralgia Outline ScriptDocument4 pagesTrigeminal Neuralgia Outline ScriptRogerQuxNo ratings yet
- Trigeminal Neura L Gi A and Its Management: Rahul Sharma Dept of OMFS DAV Dental CollegeDocument79 pagesTrigeminal Neura L Gi A and Its Management: Rahul Sharma Dept of OMFS DAV Dental CollegeIsyana Khaerunisa100% (2)
- NerualgiaDocument7 pagesNerualgiaKabirNo ratings yet
- Orofacial PainDocument40 pagesOrofacial Painghazy100% (1)
- Trigeminal NeuralgiaDocument15 pagesTrigeminal NeuralgiaMihir Patel75% (4)
- Trigeminal Neuralgia: DR Tay Kwang Hui Dept of Anaesthesia 08 January 2011Document40 pagesTrigeminal Neuralgia: DR Tay Kwang Hui Dept of Anaesthesia 08 January 2011Shalim BagusNo ratings yet
- Trigeminal NeuralgiaDocument35 pagesTrigeminal NeuralgiaMahad abuukarNo ratings yet
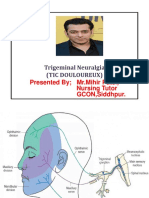
- Trigeminal Neuralgia (Tic Douloureux) : Presented by MR - Mihir Patel, Nursing Tutor GCON, SiddhpurDocument15 pagesTrigeminal Neuralgia (Tic Douloureux) : Presented by MR - Mihir Patel, Nursing Tutor GCON, Siddhpurandreas kevinNo ratings yet
- Trigeminal Neuralgia: Amithbabu.C.B Mscd-EndoDocument18 pagesTrigeminal Neuralgia: Amithbabu.C.B Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- Trigeminal NeuralgiaDocument27 pagesTrigeminal Neuralgiamelencio olivasNo ratings yet
- Neurolgy 2Document92 pagesNeurolgy 2Noura RihanNo ratings yet
- Trigeminal NeuralgiaDocument5 pagesTrigeminal Neuralgiawidad syairoziNo ratings yet
- Facialpain 150204113108 Conversion Gate01Document51 pagesFacialpain 150204113108 Conversion Gate01Muhammad IrfanNo ratings yet
- Neuralgia TrigeminalDocument5 pagesNeuralgia TrigeminalcantikarevieraNo ratings yet
- Diseases of Nerves and MusclesDocument46 pagesDiseases of Nerves and MusclesAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Neurological Disturbances of FaceDocument33 pagesNeurological Disturbances of FaceDrMuskan AroraNo ratings yet
- Trigeminal NeuralgiaDocument48 pagesTrigeminal NeuralgiaSonia Bhansali100% (4)
- Trigeminal NeurlgiaDocument5 pagesTrigeminal NeurlgiaAnonymous V1tCwPHlDNo ratings yet
- Trigeminal Neuralgia Overview: Sleep Anxiety Depression Malnutrition SuicidalDocument57 pagesTrigeminal Neuralgia Overview: Sleep Anxiety Depression Malnutrition SuicidalAmy Rose EugenioNo ratings yet
- Management of Patients With Neurologic DisordersDocument9 pagesManagement of Patients With Neurologic DisordersJames Felix Gallano GalesNo ratings yet
- Acc 61 - Supp2 96Document7 pagesAcc 61 - Supp2 96intermediosamberesNo ratings yet
- Presentation Cranial Nerve DisordersDocument30 pagesPresentation Cranial Nerve DisordersSania SaeedNo ratings yet
- TrigeminalNeuralgiaPracticeEssentials, Background, Anatomy 1700148132569Document9 pagesTrigeminalNeuralgiaPracticeEssentials, Background, Anatomy 1700148132569esthersilingi12No ratings yet
- HeadacheDocument33 pagesHeadacheMpanso Ahmad AlhijjNo ratings yet
- Trigeminal NeuralgiaDocument6 pagesTrigeminal NeuralgiamimirkuNo ratings yet
- 15.trigeminal NeuralgiaDocument25 pages15.trigeminal NeuralgiaBhakti WashilkarNo ratings yet
- Neuropathies: Mrs. Keerthana.B Assistant Professor MSN, PSG ConDocument65 pagesNeuropathies: Mrs. Keerthana.B Assistant Professor MSN, PSG ConKeerthana BNo ratings yet
- Cns الجديدةDocument9 pagesCns الجديدةlyli Star AngeloNo ratings yet
- What Is Trigeminal NeuralgiaDocument3 pagesWhat Is Trigeminal NeuralgiakewpietheresaNo ratings yet
- Trigeminal NeuralgiaDocument7 pagesTrigeminal NeuralgiaEricsonMitraNo ratings yet
- Facial Pain:: Types of NeuralgiaDocument7 pagesFacial Pain:: Types of NeuralgiaNada BrassnNo ratings yet
- Penyakit MeniereDocument25 pagesPenyakit MeniereMuhammad Budiman Irpan BachtiarNo ratings yet
- Headache: Dep. of Neurology, General Hospital of Ningxia Medical University Cell Phone:13709599000Document50 pagesHeadache: Dep. of Neurology, General Hospital of Ningxia Medical University Cell Phone:13709599000ArvindhanNo ratings yet
- Multiple SclerosisDocument24 pagesMultiple SclerosisKulgaurav RegmiNo ratings yet
- TRIGEMINALDocument12 pagesTRIGEMINALapi-19916399No ratings yet
- Intralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?From EverandIntralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?No ratings yet
- Neurological Disorders of Maxillofacial Region.Document59 pagesNeurological Disorders of Maxillofacial Region.Doktor AyeşhaNo ratings yet
- Headache - A Quick TutorialDocument7 pagesHeadache - A Quick TutorialLeilia FibrianasariNo ratings yet
- Disorder of Neuromuscular Junction: Myasthenia Gravis and Lambert-Eaton Myasthenic SyndromeDocument36 pagesDisorder of Neuromuscular Junction: Myasthenia Gravis and Lambert-Eaton Myasthenic SyndromePraneethaNo ratings yet
- Management of Intracranial Pain: Aliah Shivaan I Sara Anne William Sailo Aisyah Jayson Yuen Alice Hafizah Archan ADocument63 pagesManagement of Intracranial Pain: Aliah Shivaan I Sara Anne William Sailo Aisyah Jayson Yuen Alice Hafizah Archan AWilliam OngNo ratings yet
- Neurological DisordersDocument20 pagesNeurological DisordersEdil M JamaNo ratings yet
- Wilhour-Nahas2018 Article The NeuralgiasDocument8 pagesWilhour-Nahas2018 Article The NeuralgiasCamilo Benavides BurbanoNo ratings yet
- Case 1Document12 pagesCase 1Denisa-Alexandra MănăstireanuNo ratings yet
- Pharmacotherapeuticsiii Assignment-Ii - Neuralgias: By-Shaheestha Tabasum Roll No: 18111T0014 Pharmd 4thyrDocument439 pagesPharmacotherapeuticsiii Assignment-Ii - Neuralgias: By-Shaheestha Tabasum Roll No: 18111T0014 Pharmd 4thyrtabasum shahhNo ratings yet
- Neurological DiseasesDocument91 pagesNeurological Diseasesrabia khalidNo ratings yet
- Lecture 06.8 (Dr. Althekair's Lecture) - Common Peripheral NeuropathiesDocument68 pagesLecture 06.8 (Dr. Althekair's Lecture) - Common Peripheral NeuropathiesmaodNo ratings yet
- Drug Study LidocaineDocument15 pagesDrug Study LidocaineFrancym R. BatengaNo ratings yet
- Q1.Flaccid Paresis: Diagnostical VariantsDocument47 pagesQ1.Flaccid Paresis: Diagnostical VariantsNelson OduorNo ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- Trigeminal Neuralgia: A Beginner's 3-Step Quick Start Guide to Managing TB Through Diet, With Sample RecipesFrom EverandTrigeminal Neuralgia: A Beginner's 3-Step Quick Start Guide to Managing TB Through Diet, With Sample RecipesNo ratings yet
- MigraineDocument38 pagesMigraineManju PriyaNo ratings yet
- Acute HeadacheDocument16 pagesAcute Headachebabon3No ratings yet
- Health Optimizing Physical Education Quarter 3 - Module 5 DanceDocument22 pagesHealth Optimizing Physical Education Quarter 3 - Module 5 DanceRey Jay Baratos80% (5)
- Separate Hard Lumps, Like Nuts: Constipated Stool - Types 1 or 2 Diarrheal Stool - Types 6 or 7Document2 pagesSeparate Hard Lumps, Like Nuts: Constipated Stool - Types 1 or 2 Diarrheal Stool - Types 6 or 7nicky_lauw5885No ratings yet
- Deadman Mazin Al Khafaji Kevin BakerDocument34 pagesDeadman Mazin Al Khafaji Kevin Bakermelho.cottonNo ratings yet
- Mayo Clinic BPPVDocument4 pagesMayo Clinic BPPVCS NarayananNo ratings yet
- Stroke SyndromesDocument2 pagesStroke SyndromesRyan TownsendNo ratings yet
- Symptoms of Flu: Share On PinterestDocument4 pagesSymptoms of Flu: Share On Pinterestdinesh11rNo ratings yet
- CartiDocument3 pagesCartiGeorgiana CotarceaNo ratings yet
- Anorexia and BulimiaDocument4 pagesAnorexia and BulimiaSunny Dayanna Gelves BolañoNo ratings yet
- Abdominal Pains in Children Under 12Document5 pagesAbdominal Pains in Children Under 12clubsanatateNo ratings yet
- ReferencesDocument3 pagesReferencesTuti AsmaraNo ratings yet
- Medical Masseur Kezdő, HaladóDocument38 pagesMedical Masseur Kezdő, HaladóMagdolna BednárNo ratings yet
- Case 10 (Post-Operative Pain Management & Complication)Document10 pagesCase 10 (Post-Operative Pain Management & Complication)ReddyNo ratings yet
- Anesthesia Side EffectsDocument10 pagesAnesthesia Side EffectsPADAYON MEDISINANo ratings yet
- 41 Glasgow Coma Scale FormDocument2 pages41 Glasgow Coma Scale FormAina HaravataNo ratings yet
- B PPVDocument22 pagesB PPVNikki M. ArapolNo ratings yet
- 19 - Symptoms, Signs and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified (R00-R99) - 1Document23 pages19 - Symptoms, Signs and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified (R00-R99) - 1Wardatul MukhlishohNo ratings yet
- Cyclic Vomiting SyndromeDocument6 pagesCyclic Vomiting SyndromeSusan LasleyNo ratings yet
- Neuropathic Pain ScalesDocument5 pagesNeuropathic Pain ScalesStarry NadiaNo ratings yet
- Patient Health Questionnaire-15: Physical SymptomsDocument1 pagePatient Health Questionnaire-15: Physical SymptomssorcNo ratings yet
- Reading Test Unit 6Document3 pagesReading Test Unit 6MATEO camposNo ratings yet
- ReferensiDocument4 pagesReferensiBayuAjiWicaksonoNo ratings yet
- Chelidonim VS NuxvomDocument3 pagesChelidonim VS Nuxvomtakne_007No ratings yet
- 1506359236-Assignment 13 - Diagnosing Schizophrenia and Other Psychotic DisordersDocument4 pages1506359236-Assignment 13 - Diagnosing Schizophrenia and Other Psychotic DisordersRita Prince0% (1)
- Acute Limb Compartment Syndrome: Observation ChartDocument2 pagesAcute Limb Compartment Syndrome: Observation CharttioNo ratings yet
- Alice in Wonderland SyndromeDocument4 pagesAlice in Wonderland SyndromerakeshjakharNo ratings yet
- Spicy Foods Chili Peppers Ginger in Treatment of Migraine Headaches Byamos GelbardDocument1 pageSpicy Foods Chili Peppers Ginger in Treatment of Migraine Headaches Byamos Gelbardpavans25No ratings yet
- Stroke NSTP ReportDocument22 pagesStroke NSTP ReportMenard NavaNo ratings yet
- Health Assessment Form - BHERTDocument2 pagesHealth Assessment Form - BHERTPoblacion 04 San LuisNo ratings yet