You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Evaluation of The Epa Selected Remedy For Operable Unit-1 (Ou-1) - AppendixDocument78 pagesEvaluation of The Epa Selected Remedy For Operable Unit-1 (Ou-1) - AppendixEnformableNo ratings yet
- Evaluation of The Selected Remedy For Operable Unit-1 at The West Lake Landfill, July 20, 2016Document10 pagesEvaluation of The Selected Remedy For Operable Unit-1 at The West Lake Landfill, July 20, 2016EnformableNo ratings yet
- Exhibit 20 - Redaction of Information Released by TEPCODocument6 pagesExhibit 20 - Redaction of Information Released by TEPCOEnformableNo ratings yet
- Exhibit 19 - Redaction of Recommendations Shared With IndustryDocument15 pagesExhibit 19 - Redaction of Recommendations Shared With IndustryEnformableNo ratings yet
- Pages From C147359-02X - March 17th, 2011 - Special Lawyers Group Tackled Legal Issues Arising From Fukushima Disaster Response For White HouseDocument8 pagesPages From C147359-02X - March 17th, 2011 - Special Lawyers Group Tackled Legal Issues Arising From Fukushima Disaster Response For White HouseEnformableNo ratings yet
- Exhibit 14 - Redaction of OPA Talking PointsDocument11 pagesExhibit 14 - Redaction of OPA Talking PointsEnformableNo ratings yet
- Exhibit 21 - Sample Redacted MaterialsDocument29 pagesExhibit 21 - Sample Redacted MaterialsEnformableNo ratings yet
- Pages From C147216-02X - March 19th, 2011 - NRC NARAC Models of Fukushima Daiichi Disaster Did Not Model All Available RadionuclidesDocument14 pagesPages From C147216-02X - March 19th, 2011 - NRC NARAC Models of Fukushima Daiichi Disaster Did Not Model All Available RadionuclidesEnformableNo ratings yet
- Pages From C147216-02X - March 15th, 2011 - Navy Tried To Get Dosimeters For All Sailors On USS Ronald Reagan After Fukushima DisasterDocument50 pagesPages From C147216-02X - March 15th, 2011 - Navy Tried To Get Dosimeters For All Sailors On USS Ronald Reagan After Fukushima DisasterEnformableNo ratings yet
- Exhibit 7 - Bruce Watson CommunicationsDocument64 pagesExhibit 7 - Bruce Watson CommunicationsEnformableNo ratings yet
- Exhibit 17 - Redaction of Payroll InformationDocument7 pagesExhibit 17 - Redaction of Payroll InformationEnformableNo ratings yet
- Exhibit 16 - Redaction of Material Derived From Public DocumentsDocument9 pagesExhibit 16 - Redaction of Material Derived From Public DocumentsEnformableNo ratings yet
- Exhibit 18 - Redaction of Information Shared With IndustryDocument17 pagesExhibit 18 - Redaction of Information Shared With IndustryEnformableNo ratings yet
- Exhibit 11 - Redacted Presentation From Nuclear Energy System Safety Division of JNESDocument26 pagesExhibit 11 - Redacted Presentation From Nuclear Energy System Safety Division of JNESEnformableNo ratings yet
- Exhibit 12 - Potential Near-Term Options To Mitigate Contaminated Water in Japan's Fukushima Daiichi Nuclear PlantDocument57 pagesExhibit 12 - Potential Near-Term Options To Mitigate Contaminated Water in Japan's Fukushima Daiichi Nuclear PlantEnformableNo ratings yet
- Exhibit 9 - Redaction of NRC PresentationDocument12 pagesExhibit 9 - Redaction of NRC PresentationEnformableNo ratings yet
- Exhibit 13 - Redacted Generic EmailDocument28 pagesExhibit 13 - Redacted Generic EmailEnformableNo ratings yet
- Exhibit 15 - Redaction of Time-Off RequestDocument1 pageExhibit 15 - Redaction of Time-Off RequestEnformableNo ratings yet
- Exhibit 8 - Document Search DOE Doc EGG-M-09386 CONF-860724-14Document19 pagesExhibit 8 - Document Search DOE Doc EGG-M-09386 CONF-860724-14EnformableNo ratings yet
- Exhibit 1 - Redaction of Answers To Bill Dedman's QuestionsDocument10 pagesExhibit 1 - Redaction of Answers To Bill Dedman's QuestionsEnformableNo ratings yet
- Exhibit 6 - PMT Request of Realistic Up-To-Date Estimation of Source TermsDocument6 pagesExhibit 6 - PMT Request of Realistic Up-To-Date Estimation of Source TermsEnformableNo ratings yet
- Exhibit 10 - Redacted CommunicationsDocument3 pagesExhibit 10 - Redacted CommunicationsEnformableNo ratings yet
- March 21st, 2011 - A Delta Pilot's Perspective On His Approach To Tokyo in The Wake of The March 11th Earthquake - Pages From C146330-02X - Partial - Group Letter DO.-2Document2 pagesMarch 21st, 2011 - A Delta Pilot's Perspective On His Approach To Tokyo in The Wake of The March 11th Earthquake - Pages From C146330-02X - Partial - Group Letter DO.-2EnformableNo ratings yet
- Exhibit 5 - Comparison of Intervention Levels For Different CountriesDocument11 pagesExhibit 5 - Comparison of Intervention Levels For Different CountriesEnformableNo ratings yet
- Exhibit 4 - Answers From DOE in Response To TEPCODocument18 pagesExhibit 4 - Answers From DOE in Response To TEPCOEnformableNo ratings yet
- March 14th, 2011 - TEPCO Requests US Embassy Help Extinguish Fire at Unit 4 - Pages From C146301-02X - Group DK-18Document2 pagesMarch 14th, 2011 - TEPCO Requests US Embassy Help Extinguish Fire at Unit 4 - Pages From C146301-02X - Group DK-18EnformableNo ratings yet
- Exhibit 3 - Documents Shared With International PartiesDocument19 pagesExhibit 3 - Documents Shared With International PartiesEnformableNo ratings yet
- Exhibit 2 - Agendas Largely RedactedDocument13 pagesExhibit 2 - Agendas Largely RedactedEnformableNo ratings yet
- March 17th, 2011 - Hopefully This Would Not Happen Here - Pages From C146257-02X - Group DL. Part 1 of 1-2Document1 pageMarch 17th, 2011 - Hopefully This Would Not Happen Here - Pages From C146257-02X - Group DL. Part 1 of 1-2EnformableNo ratings yet
- March 22nd, 2011 - Core Melt at Fukushima Unit 1 From 11 To 12 March 2011 - Pages From C146301-02X - Group DK-30Document3 pagesMarch 22nd, 2011 - Core Melt at Fukushima Unit 1 From 11 To 12 March 2011 - Pages From C146301-02X - Group DK-30EnformableNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Biology Project 2015Document40 pagesBiology Project 2015vivaan50% (12)
- NUS Engineering Annual Report 2016Document23 pagesNUS Engineering Annual Report 2016Glenden KhewNo ratings yet
- 10 Anos Cross Trial Jco2021Document11 pages10 Anos Cross Trial Jco2021alomeletyNo ratings yet
- 14 Cancer Symptoms Women Ignore - 3Document1 page14 Cancer Symptoms Women Ignore - 3Meidi RaniNo ratings yet
- Persuasive Essay PDFDocument5 pagesPersuasive Essay PDFapi-603689898No ratings yet
- Secrets of The Billionaire Mind v1.0Document101 pagesSecrets of The Billionaire Mind v1.0Debanik GhoshNo ratings yet
- Penile Squamous Cell CarcinomaDocument64 pagesPenile Squamous Cell CarcinomaTres De GuzmanNo ratings yet
- MeningiomaDocument4 pagesMeningiomaHariyehNo ratings yet
- First Aid 2015 Pages AddedDocument11 pagesFirst Aid 2015 Pages AddedNicole WilliamNo ratings yet
- Literature Review On Cervical Cancer PDFDocument5 pagesLiterature Review On Cervical Cancer PDFafmzmxkayjyoso100% (1)
- Ten Reasons To Stop CookingDocument15 pagesTen Reasons To Stop CookingTomuta Adrian Marius100% (1)
- Journal of Infection and Public Health: Tanzila SabaDocument16 pagesJournal of Infection and Public Health: Tanzila SabaprnjanNo ratings yet
- Adenoma 2020Document11 pagesAdenoma 2020Residentes AudiologiaNo ratings yet
- St. Paul University's 4th Quarter Health Education 7 DIPDocument8 pagesSt. Paul University's 4th Quarter Health Education 7 DIPClarisse-joan Bumanglag GarmaNo ratings yet
- Sample Focus Group Moderator's GuideDocument4 pagesSample Focus Group Moderator's GuideDivyesh ChadotraNo ratings yet
- Cervical Cancer Screening ThesisDocument6 pagesCervical Cancer Screening Thesisbk1svxmr100% (3)
- Hereditary Tumor Syndromes With Skin InvolvementDocument7 pagesHereditary Tumor Syndromes With Skin Involvementghinan jamilahNo ratings yet
- A Cancer Care Ontario Consensus Based OrganizationDocument11 pagesA Cancer Care Ontario Consensus Based OrganizationAhmedNo ratings yet
- Download ebook Medical Secrets Pdf full chapter pdfDocument67 pagesDownload ebook Medical Secrets Pdf full chapter pdfregina.white324100% (23)
- The Impact of Physical Activities On The Health of AdultsDocument12 pagesThe Impact of Physical Activities On The Health of AdultsJUNAID AHMEDNo ratings yet
- Kriteria 4 Tabel 10 18 - 08 - 2022Document23 pagesKriteria 4 Tabel 10 18 - 08 - 2022harsya Yuli RachmantoNo ratings yet
- Kidney Cancer Symptoms, Risk Factors, and TreatmentDocument30 pagesKidney Cancer Symptoms, Risk Factors, and Treatmentsongkyo100% (1)
- Cervical Polyp 12345Document13 pagesCervical Polyp 12345Osama Edris Hama SamanNo ratings yet
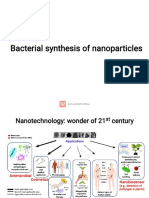
- Bacterial Synthesis of Nanoparticles for Biomedical ApplicationsDocument16 pagesBacterial Synthesis of Nanoparticles for Biomedical ApplicationsDibyajyoti20 Das4001No ratings yet
- Opioids, Pain, and FearDocument3 pagesOpioids, Pain, and FearlucianaclarkNo ratings yet
- Rectosigmoid Carcinoma: Department of SurgeryDocument19 pagesRectosigmoid Carcinoma: Department of SurgeryHana FauziNo ratings yet
- Eyelid Tumor Characteristics and Accuracy of Clinical Diagnosis Against Anatomical Pathology ResultsDocument6 pagesEyelid Tumor Characteristics and Accuracy of Clinical Diagnosis Against Anatomical Pathology ResultssantiNo ratings yet
- Oncology NursingDocument12 pagesOncology NursingDick Morgan Ferrer80% (5)
- Head NeckDocument254 pagesHead Neckdrsajal100% (1)
- Problems in Digestion, Metabolism and Elimination/Nutrition: Nursing Facts in BriefDocument2 pagesProblems in Digestion, Metabolism and Elimination/Nutrition: Nursing Facts in BriefAdrienne SumarinasNo ratings yet