Cardiogenic Shock
Management Strategies
Cardiogenic Shock
Management Strategies
Fayaz Shawl, M.D., F.A.C.C.
Director Interventional Cardiology
Washington Adventist Hospital - Takoma Park,
Maryland
Clinical Professor of Medicine
Director of Interventional Cardiovascular Medicine
George Washington University - Washington, D.C.
Fayaz Shawl, M.D., F.A.C.C.
Director Interventional Cardiology
Washington Adventist Hospital - Takoma Park,
Maryland
Clinical Professor of Medicine
Director of Interventional Cardiovascular Medicine
George Washington University - Washington, D.C.
CIT 2007
Beijing International Convention Center, China
March 29 April 1 , 2007
CIT 2007
Beijing International Convention Center, China
March 29 April 1 , 2007
Research/Grant Support
Medtronic
Abbott Vascular
Cordis Corp. (J & J)
Carotid Proctoring Program
Guidant/Abbott Vascular
Cordis Corp. (J & J)
Research/Grant Support
Medtronic
Abbott Vascular
Cordis Corp. (J & J)
Carotid Proctoring Program
Guidant/Abbott Vascular
Cordis Corp. (J & J)
Within the past 12 months, I or my spouse/partner have had a
financial interest/arrangement or affiliation with the organization(s)
listed below.
Within the past 12 months, I or my spouse/partner have had a
financial interest/arrangement or affiliation with the organization(s)
listed below.
Conflict of Interest Statement
Fayaz Shawl, MD
Conflict of Interest Statement
Fayaz Shawl, MD
Definition of Cardiogenic Shock
Definition of Cardiogenic Shock
SBP < 90 mmHg for 1 hr that is:
Unresponsive to fluids alone
Secondary to myocardial dysfunction, or
associated with signs of hypoperfusion, or
Associated with CI < 2.2 L/mm/m
2
and PCWP > 18
mmHg, or
Associated with death
SBP < 90 mmHg for 1 hr that is:
Unresponsive to fluids alone
Secondary to myocardial dysfunction, or
associated with signs of hypoperfusion, or
Associated with CI < 2.2 L/mm/m
2
and PCWP > 18
mmHg, or
Associated with death
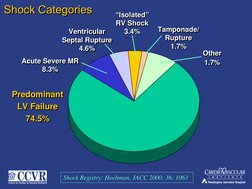
Shock Categories
Shock Categories
Predominant
LV Failure
74.5%
Predominant
LV Failure
74.5%
Acute Severe MR
8.3%
Acute Severe MR
8.3%
Ventricular
Septal Rupture
4.6%
Ventricular
Septal Rupture
4.6%
Isolated
RV Shock
3.4%
Isolated
RV Shock
3.4%
Tamponade/
Rupture
1.7%
Tamponade/
Rupture
1.7%
Other
1.7%
Other
1.7%
Shock Registry: Hochman, JACC 2000; 36: 1063
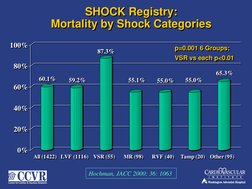
60.1%
59.2%
87.3%
55.1%
55.0%
55.0%
65.3%
0%
20%
40%
60%
80%
100%
All (1422) LVF (1116) VSR (55) MR (98) RVF (40) Tamp (20) Other (95)
60.1%
59.2%
87.3%
55.1%
55.0%
55.0%
65.3%
0%
20%
40%
60%
80%
100%
All (1422) LVF (1116) VSR (55) MR (98) RVF (40) Tamp (20) Other (95)
SHOCK Registry:
Mortality by Shock Categories
SHOCK Registry:
Mortality by Shock Categories
Hochman, JACC 2000; 36: 1063
p=0.001 6 Groups;
VSR vs each p<0.01
p=0.001 6 Groups;
VSR vs each p<0.01
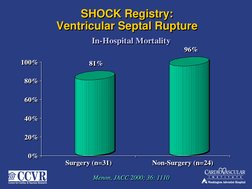
81%
96%
0%
20%
40%
60%
80%
100%
Surgery (n=31) Non-Surgery (n=24)
In-Hospital Mortality
81%
96%
0%
20%
40%
60%
80%
100%
Surgery (n=31) Non-Surgery (n=24)
In-Hospital Mortality
SHOCK Registry:
Ventricular Septal Rupture
SHOCK Registry:
Ventricular Septal Rupture
Menon, JACC 2000; 36: 1110
Menon, JACC 2000; 36: 1110
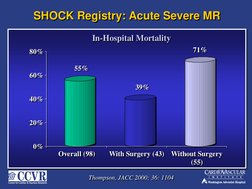
55%
39%
71%
0%
20%
40%
60%
80%
Overall (98) With Surgery (43) Without Surgery
(55)
In-Hospital Mortality
55%
39%
71%
0%
20%
40%
60%
80%
Overall (98) With Surgery (43) Without Surgery
(55)
In-Hospital Mortality
SHOCK Registry: Acute Severe MR
SHOCK Registry: Acute Severe MR
Thompson, JACC 2000; 36: 1104
Thompson, JACC 2000; 36: 1104
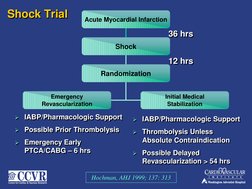
Acute Myocardial Infarction
Shock
Randomization
Emergency
Revascularization
Initial Medical
Stabilization
12 hrs
12 hrs
Shock Trial
Shock Trial
36 hrs
36 hrs
IABP/Pharmacologic Support
Possible Prior Thrombolysis
Emergency Early
PTCA/CABG 6 hrs
IABP/Pharmacologic Support
Possible Prior Thrombolysis
Emergency Early
PTCA/CABG 6 hrs
IABP/Pharmacologic Support
Thrombolysis Unless
Absolute Contraindication
Possible Delayed
Revascularization > 54 hrs
IABP/Pharmacologic Support
Thrombolysis Unless
Absolute Contraindication
Possible Delayed
Revascularization > 54 hrs
Hochman, AHJ 1999; 137: 313
SHOCK Trial:
Emergency Revascularization Group (N=152)
SHOCK Trial:
Emergency Revascularization Group (N=152)
Angio
n=147 (97%)
Revascularization
n=132 (87%)
No Revascularization
n=15 (13%)
No Angio
n=5 (3%)
PTCA
n=75 (49%)
0.9 hrs
CABG*
n=57 (38%)
2.7 hrs
* Includes 5 late CABG
(23 431 hrs.)
* Includes 5 late CABG
(23 431 hrs.)
Coronary Angio/Revascularization
Coronary Angio/Revascularization
1%
3%
13%
8%
22%
24%
64% 65%
23%
18%
0%
10%
20%
30%
40%
50%
60%
70%
No Disease Single Vessel
Disease
2-Vessel
Disease
3-Vessel
Disease
Left Main
Disease
ERV (n=143)
IMS (n=96)
SHOCK Trial:
Angiographic Findings
SHOCK Trial:
Angiographic Findings
Hochman, NEJM 1999; 341: 625
Hochman, NEJM 1999; 341: 625
SHOCK Trial:
Long-term Survival (N = 302)
SHOCK Trial:
Long-term Survival (N = 302)
SHOCK Trial:
30-Day Mortality By PTCA Success
SHOCK Trial:
30-Day Mortality By PTCA Success
38%
78%
39%
100%
34%
65%
0%
20%
40%
60%
80%
100%
I
n
c
i
d
e
n
c
e
</=50% Stenosis TIMI 2/3 Flow TIMI 3 Flow
ERV Group (N=81)
Successful
Unsuccessful
38%
78%
39%
100%
34%
65%
0%
20%
40%
60%
80%
100%
I
n
c
i
d
e
n
c
e
</=50% Stenosis TIMI 2/3 Flow TIMI 3 Flow
ERV Group (N=81)
Successful
Unsuccessful
All p<0.01
All p<0.01
Sanborn, Circulation 1999, 100: 1-370
Sanborn, Circulation 1999, 100: 1-370
SHOCK Trial:
ERV Group
SHOCK Trial:
ERV Group
PCI Increases Mortality in Elderly
( 75 yrs) Shock Patients
PCI Increases Mortality in Elderly
( 75 yrs) Shock Patients
53.1
56.3
75
79.2
0
20
40
60
80
100
D
e
a
t
h
s
(
%
P
t
s
)
30 Days 6 Months
Medical
Revasc.
53.1
56.3
75
79.2
0
20
40
60
80
100
D
e
a
t
h
s
(
%
P
t
s
)
30 Days 6 Months
Medical
Revasc.
p < .01
p < .01
p = .003
p = .003
Hochman, NEJM 1999; 341: 625-34
Hochman, NEJM 1999; 341: 625-34
PCI Increases Mortality in Elderly
( 75 yrs) Shock Patients
PCI Increases Mortality in Elderly
( 75 yrs) Shock Patients
77%
63%
53%
47%
0%
10%
20%
30%
40%
50%
60%
70%
80%
No IABP / Lytic IABP only Lytic only IABP + Lytic
In-Hospital Mortality
77%
63%
53%
47%
0%
10%
20%
30%
40%
50%
60%
70%
80%
No IABP / Lytic IABP only Lytic only IABP + Lytic
In-Hospital Mortality
p < 0.001
p < 0.001
Sanborn, JACC 2000; 36: 1123
Sanborn, JACC 2000; 36: 1123
Shock Non STEMI Shock Registry
Jacobs, et al. JACC 2000; 36:1091
Shock Non STEMI Shock Registry
Jacobs, et al. JACC 2000; 36:1091
1,190 CS
881 Study Group
STEMI
(n=729)
Non STEMI
(n=152)
5 missing ECG data
304 mechanical complications
5 missing ECG data
304 mechanical complications
Mortality 63%
Mortality 63%
Mortality 60%
Mortality 60%
MANAGEMENT STRATEGIES
CARDIOGENIC SHOCK
MANAGEMENT STRATEGIES
CARDIOGENIC SHOCK
Dont Panic !!!
BP support ; Airway
Call for an extra-hand
Be Quick but be steady
Dont Panic !!!
BP support ; Airway
Call for an extra-hand
Be Quick but be steady
ACC/AHA Guidelines for STEMI 2004:
Treatment of Low-Output State/Cardiogenic Shock
ACC/AHA Guidelines for STEMI 2004:
Treatment of Low-Output State/Cardiogenic Shock
Class I
Fluids, inotropic support, IABP, echo, PA and art line
monitoring
Mechanical reperfusion with PCI or CABG if age < 75,
early shock (< 18 hrs)
Surgical correction of mechanical defects
Fibrinolytic therapy if not suitable for invasive approach
Class IIa
Early revasc. In selected patients 75 yrs old if good prior
functional status and present early
Class III Not recommended or contraindicated
blockers
Calcium channel antagonists
Class I
Fluids, inotropic support, IABP, echo, PA and art line
monitoring
Mechanical reperfusion with PCI or CABG if age < 75,
early shock (< 18 hrs)
Surgical correction of mechanical defects
Fibrinolytic therapy if not suitable for invasive approach
Class IIa
Early revasc. In selected patients 75 yrs old if good prior
functional status and present early
Class III Not recommended or contraindicated
blockers
Calcium channel antagonists
Cardiogenic Shock : Management
Preventive measures prior to PCI
Cardiogenic Shock : Management
Preventive measures prior to PCI
Assess Right Heart Pressures
Maintain adequate airway- O2 Saturation
Prophylactic Temporary Pacemaker ( Brady.)
IABP
LV Assist Devices : ( unstable rhythm )
Assess Right Heart Pressures
Maintain adequate airway- O2 Saturation
Prophylactic Temporary Pacemaker ( Brady.)
IABP
LV Assist Devices : ( unstable rhythm )
Management Strategies
Pharmacological
Adenosine ( reduce reperfusion Injury)
2mg I/C through PTCA balloon distal
to occlusion prior to Angioplasty
Improved Survival, TIMI grade flow
Marzilli et al , Cir 2000
ACC/AHA Guidelines for STEMI 2004:
Treatment of Low-Output State/Cardiogenic Shock
ACC/AHA Guidelines for STEMI 2004:
Treatment of Low-Output State/Cardiogenic Shock
Low Output Cardiogenic Shock
Check Blood Pressure
Systolic BP
70-100 mm Hg
NO signs/sx
of shock
Systolic BP
70-100 mm Hg
Signs/sx
of shock
Systolic BP
< 70 mm Hg
Signs/sx
of shock
Systolic BP
> 100 mm Hg
NTG
10-20 mcg
/min IV
Dobutamine
2-20 mcg/kg
/min IV
Norepinephrine
0.5-30 mcg
/min IV
Dopamine
5-15 mcg/kg
/min IV
Management Strategies
Mechanical
Approved PercutaneousLVADs
1. IABP
2. CPS
3. Tandem Heart
Investigational PercutaneousLVADs
1.A- Med Device
2. Impella Device
Relative Merits of Percutaneous LVAD
Relative Merits of Percutaneous LVAD
IABP:
small, very easy to use, inexpensive-
needs stable rhythm)
CPS:
Complete Support , not dependant on
intrinsic rhythm ( large catheters,
complex,
IABP:
small, very easy to use, inexpensive-
needs stable rhythm)
CPS:
Complete Support , not dependant on
intrinsic rhythm ( large catheters,
complex,
Relative Merits of Percutaneous LVAD
Relative Merits of Percutaneous LVAD
Tandem heart:
Complete support , not dependant on
intrinsic rhythm, complete unloading (21f,
need transseptal & RV function)
Impella Device:
Complete support, easy to use, complete
support, ( 12- 20 F), needs RV function,
Expensive, not with aortic valve stenosis
Tandem heart:
Complete support , not dependant on
intrinsic rhythm, complete unloading (21f,
need transseptal & RV function)
Impella Device:
Complete support, easy to use, complete
support, ( 12- 20 F), needs RV function,
Expensive, not with aortic valve stenosis
Percutaneous LVAD
Percutaneous LVAD
71 yr M, AMI CS - 3 V CAD
71 yr M, AMI CS - 3 V CAD
PCI to the Culprit Vessel- LAD
78 M, C.S, Non- ST
78 M, C.S, Non- ST
9 month Follow-Up angio
73 Yr AMI-CS Post Thrombolytic
45 yr woman, CS followed by CA
Pulmonary capillary wedge tracing before
and after PCI to RCA
Pulmonary capillary wedge tracing before
and after PCI to RCA
RAO projection @
presentation (A & B)
and after
angioplasty (C & D)
End-systolic frame
(B) shows 3+ mitral
regurgitation into
the left atrium
(arrows); after
angioplasty, no
mitral regurgitation
is evident (D).
RAO projection @
presentation (A & B)
and after
angioplasty (C & D)
End-systolic frame
(B) shows 3+ mitral
regurgitation into
the left atrium
(arrows); after
angioplasty, no
mitral regurgitation
is evident (D).
End-diastolic and end-systolic ventriculograms
End-diastolic and end-systolic ventriculograms
Shawl,FA et al JACC 1989:14:967
Management of Cardiogenic Shock
Management of Cardiogenic Shock
Quick Echo Doppler to r/o mechanical defects
Swan to determine filling pressures, CO and SVR
guide therapy
Maintain atrial kick with AV sequential pacer if
brady, cardioversion if Afib ,augments CO by 30%
Age > 75 with CS, Swan, IABP (consider
emergency cath if recent onset shock, living
independently, etc.)
Age < 75 Emergency IABP and cath
Limit contrast to avoid renal failure (pre- Mucomyst )
Quick Echo Doppler to r/o mechanical defects
Swan to determine filling pressures, CO and SVR
guide therapy
Maintain atrial kick with AV sequential pacer if
brady, cardioversion if Afib ,augments CO by 30%
Age > 75 with CS, Swan, IABP (consider
emergency cath if recent onset shock, living
independently, etc.)
Age < 75 Emergency IABP and cath
Limit contrast to avoid renal failure (pre- Mucomyst )
Management of Cardiogenic Shock
Management of Cardiogenic Shock
PCI of suspected culprit, if no improvement
consider PCI of other critical lesions in major
vessels
Surgery recommended:
Failed PCI
3 Vessel or Left Main Disease
Mechanical defects
LAVD for continued shock
Consider cardiac transplant
PCI of suspected culprit, if no improvement
consider PCI of other critical lesions in major
vessels
Surgery recommended:
Failed PCI
3 Vessel or Left Main Disease
Mechanical defects
LAVD for continued shock
Consider cardiac transplant
Post---Management Issues
Post---Management Issues
Daily evaluation for:
Sepsis
Thrombocytopenia
Blood loss
Hemolysis
Vascular obstruction
Thrombus
Embolus
Daily evaluation for:
Sepsis
Thrombocytopenia
Blood loss
Hemolysis
Vascular obstruction
Thrombus
Embolus
Anticoagulation
PTT @ 50-70 seconds
AVOID TOO MANY
CONSULTANTS
Anticoagulation
PTT @ 50-70 seconds
AVOID TOO MANY
CONSULTANTS
THANK YOU