CHART AUDIT
FIN # 010-057-063
STAFF: Chris Beryl/Jorge Villahermosa
CN/TL: Lucia Malenab
SUBJECT
TRIAGE Components
General: together with the other
mandatory fields, these should be strictly
documented as needed
HAAD Injury and Poisoning
Mode of Arrival
YE
S
NAME:
DATE: 23/01/2014
SHIFT: Night
COMPLETE
NO N/
A
Glasgow Coma Scale (required for
trauma cases)
Trauma Activation / Scoring
(needs to specify also Mode of
Transport: Ambulance, Private
Vehicle, Police Vehicle,
Helicopter) aside from walking,
wheelchair, stretcher, carried
Case-dependent
Vital Signs (even for Code Patients);
Height/Weight
e.g. RR / min even via Bag Valve or
Mechanical Venti; HR = 0; BP = 0/0
Temperature
Assess / Tx
Pain Assessment
Primary Pain
ESI
Triage and Pre-Arrival Treatment
ED Assessment Components:
Please do this on all Acuity Levels, even
for T4/T5 as we are being audited for the
following components:
Vital Signs
Primary Pain
General do not forget the ISOLATION
PRECAUTION / STATUS
Health History I, II, III, Social Habits
Psychosocial
TB Screen if with cough complaints
Nutrition
Allergy Status
Safety
System Review
Morse Fall Risk / Humpty Dumpty
Repeat also if theres any change in
status
Pre IV cannulation
Post IV cannulation, medication, splinting,
COMMENTS
ZDENKOA, DANUSE
Review, modify, and complete postfacto while patient still in ED if not
done the first time
Review, modify, and complete postfacto while patient still in ED if not
done the first time
Bold lettered items are always
forgotten but are required to be
filled-up
Can be skipped on patients coming
in active resuscitation
(trauma/medical). Can be done
after patient has been revived
Do not forget please: Identification
Verified, ID Band Applied
Mandatory to include in HandOver: verbal AND in Malaffi
�etc.
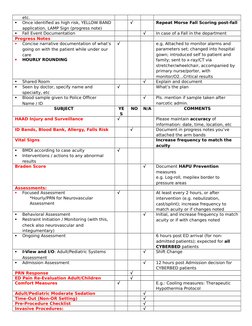
Once identified as high risk, YELLOW BAND
application, LAMP Sign (progress note)
Fall Event Documentation
Progress Notes
Concise narrative documentation of whats
going on with the patient while under our
care
HOURLY ROUNDING
Shared Room
Seen by doctor, specify name and
specialty, etc
Blood sample given to Police Officer
Name / ID
SUBJECT
HAAD Injury and Surveillance
Repeat Morse Fall Scoring post-fall
YE
S
ID Bands, Blood Bank, Allergy, Falls Risk
NO
N/A
BMDI according to case acuity
Interventions / actions to any abnormal
results
Braden Score
Assessments:
Focused Assessment
*Hourly/PRN for Neurovascular
Assessment
I-View and I/O: Adult/Pediatric Systems
Assessment
Admission Assessment
Adult/Pediatric Moderate Sedation
Time-Out (Non-OR Setting)
Pre-Procedure Checklist
Invasive Procedures:
Pls. mention if sample taken after
narcotic admin.
COMMENTS
Behavioral Assessment
Restraint Initiation / Monitoring (with this,
check also neurovascular and
integumentary)
Ongoing Assessment
PRN Response
ED Pain Re-Evaluation Adult/Children
Comfort Measures
e.g. Attached to monitor alarms and
parameters set; changed into hospital
gown; introduced self to patient and
family; sent to x-ray/CT via
stretcher/wheelchair, accompanied by
primary nurse/porter, with
monitor/O2Critical results
Explain and document
Whats the plan
Please maintain accuracy of
information: date, time, location, etc
Document in progress notes youve
attached the arm bands
Increase frequency to match the
acuity
Vital Signs
In case of a Fall in the department
Document HAPU Prevention
measures
e.g. Log-roll, mepilex border to
pressure areas
At least every 2 hours, or after
intervention (e.g. nebulization,
cast/splint); increase frequency to
match acuity or if changes noted
Initial, and increase frequency to match
acuity or if with changes noted
6 hours post ED arrival (for nonadmitted patients); expected for all
CYBERBED patients
Shift Change
12 hours post Admission decision for
CYBERBED patients
E.g.: Cooling measures: Therapeutic
Hypothermia Protocol
�Peripheral / Central Lines, Foley Cath, NGT,
ETT, etc
Consents
Care Bundles
Ventilator Associated Pneumonia
CAUTI
CLABSI
Surgical Site
Blood Administration Transfusion /
Initiation
I-View and I/O Modify your Navigator
bands to expand options aside from the
following:
Quick Views: MEWS / PEWS, Assessments,
etc.
Adult/Pediatric Systems Assessment
Patient and Family Education
Input / Output
Isolation and Order Entry Details
Patients Valuables and Belongings
Patient Transfer
Nursing Discharge Summary
Nursing Summary Hand-Over
Depart Process/ Discharge Encounter
Against Medical Advice
Document efforts of explaining risks and
convincing the patient/family
Expiration Record
Make sure it is completed
Shift Change
Mandatory
For all Admission
ED Nurse to ED Nurse; ED Nurse to
Ward Nurse / Other SEHA Facility Nurse
If Left Without Being Seen, do progress
notes also