0% found this document useful (0 votes)
393 views1 pageMedical Reimbursement Application Form
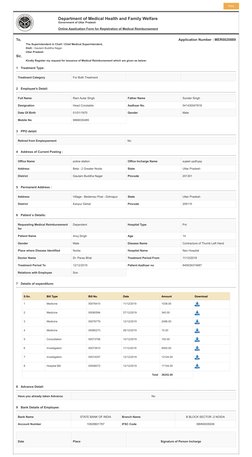
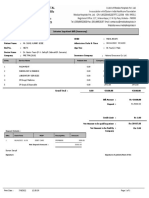
The document is an online application form submitted by Ram Autar Singh, a head constable, to the Superintendent in Chief requesting medical reimbursement for his son Anuj Singh's treatment. It provides details about the treatment category, patient and employee information, expenditure bills totaling 38,252 rupees, and bank details for reimbursement.
Uploaded by
anuj thakurCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
393 views1 pageMedical Reimbursement Application Form
The document is an online application form submitted by Ram Autar Singh, a head constable, to the Superintendent in Chief requesting medical reimbursement for his son Anuj Singh's treatment. It provides details about the treatment category, patient and employee information, expenditure bills totaling 38,252 rupees, and bank details for reimbursement.
Uploaded by
anuj thakurCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd