0% found this document useful (0 votes)
42 views1 pageVOE Form - Application
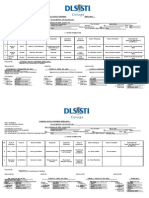
This document is a verification of employment form for nursing students. It requests information about a student's employment as a licensed nurse such as employer name, dates of employment, and number of hours worked in the last 12-24 months. For new graduates, it asks for details of their nursing program such as dates of enrollment and completion, as well as their academic standing. The completed form is to be uploaded into an application portal to verify the student's employment experience.
Uploaded by
Makala CrutchfieldCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
42 views1 pageVOE Form - Application
This document is a verification of employment form for nursing students. It requests information about a student's employment as a licensed nurse such as employer name, dates of employment, and number of hours worked in the last 12-24 months. For new graduates, it asks for details of their nursing program such as dates of enrollment and completion, as well as their academic standing. The completed form is to be uploaded into an application portal to verify the student's employment experience.
Uploaded by
Makala CrutchfieldCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd