Dig Dis Sci (2008) 53:34–40
DOI 10.1007/s10620-007-9818-0
ORIGINAL PAPER
Remifentanil Compared with Midazolam and Pethidine Sedation
During Colonoscopy: A Prospective, Randomized Study
Maria M. Manolaraki Æ Angeliki Theodoropoulou Æ Charalampos Stroumpos Æ
Emmanouil Vardas Æ Pantelis Oustamanolakis Æ Aliki Gritzali Æ
Gregorios Chlouverakis Æ Gregorios A. Paspatis
Received: 19 December 2006 / Accepted: 27 February 2007 / Published online: 3 May 2007
Ó Springer Science+Business Media, LLC 2007
Abstract
Purpose The objective of our study was to compare the Keywords Remifentanil � Colonoscopy � Midazolam �
safety and efficacy of remifentanil during colonoscopy Pethidine
with those of the standard combination of midazolam and
pethidine.
Methods One-hundred and sixteen consecutive patients Introduction
scheduled for colonoscopy were randomly assigned to
groups A or B. Patients in group A (n = 56) received Colonoscopy is one of the most commonly performed
intravenous (IV) midazolam and pethidine. Patients in outpatient procedures for diagnosis and treatment of gas-
group B (n = 60) received IV remifentanil. trointestinal disorders. Although short-lasting it can be
Results Recovery was faster in group B (0 min) than in uncomfortable for patients and a wide variety of medica-
group A (56 ± 11.3 min) (P < 0.001). There was a marked tions have been used for sedation [1]. A combination of
difference between groups B and A with regard to the time benzodiazepines and opiates (midazolam and pethidine),
of hospital discharge—28.7 ± 4.3 and 148.9 ± 34 min, the medication used most commonly by gastroenterolo-
respectively (P < 0.001). Patients in group A rated the gists, provides adequate analgesia and sedation during
procedure as comfortable, as also did those in group B. A colonoscopy [2]. Despite satisfactory comfort for most
combination of midazolam and pethidine had a greater patients undergoing colonoscopy, a combination of mi-
affect on patients’ cardiorespiratory characteristics. dazolam with opiates is not ideal. The duration of the ef-
Conclusion Remifentanil during colonoscopy provides fects of these drugs is usually longer than the time required
sufficient pain relief with better hemodynamic stability, for the procedure, and their use requires prolonged recov-
less respiratory depression, and significantly faster recov- ery, resulting in delayed hospital discharge [3]. This syn-
ery and hospital discharge than moderate sedation with ergistic sedation also increases the likelihood of ventilatory
midazolam and pethidine. depression and increases recovery time [4, 5].
Because colonoscopy requires rapid turnover of pa-
tients, an agent with rapid onset and offset of action, and
M. M. Manolaraki � A. Gritzali
Department of Anesthesiology, Benizelion General Hospital, convenient titrability of anesthetic/analgesic depth would
Heraklion-Crete, Greece be ideal. Over the last few years, there has been growing
interest in the use of propofol during endoscopic proce-
A. Theodoropoulou � C. Stroumpos � E. Vardas �
dures [2, 6–8]. Despite adequate safety data for admin-
P. Oustamanolakis � G. A. Paspatis (&)
Department of Gastroenterology, Benizelion General Hospital, istration of propofol by non-anesthesiologists, the
L.Knossou, Heraklion-Crete 71021, Greece anesthesiology community remains opposed, because the
e-mail: paspati@admin.teiher.gr drug can quickly induce deep sedation and general
anesthesia. Because there is no reversal agent for prop-
G. Chlouverakis
School of Education, University of Crete, Heraklion-Crete, ofol, the likelihood that advanced airway management
Greece techniques will be required is greater than for a combination
123
�Dig Dis Sci (2008) 53:34–40 35
of midazolam and opioids [9–12]. Most states in the Exclusion criteria were: age under 18 years, history of
USA do not, moreover, allow use of propofol by non- large-bowel surgery, pregnancy, critically ill patients
anesthesiologists. These limitations on the administration (ASA grade IV/V), patients with psychiatric/emotional
of propofol have increased clinical research on this topic, disorders, history of addiction to opiates/sedatives/alco-
with suggestions such as combining midazolam with hol, and previous adverse reactions to any medication
propofol titrated to moderate sedation or use of new agents, used in the trial. The protocol was approved by our
for example fospropofol disodium [3, 13, 14]. ethics committee.
In this study we tested the hypothesis that if pain Patients in group A (midazolam and pethidine) ini-
relief was adequate during colonoscopy, sedation would tially received 50 mg pethidine intravenously (IV). Ten
no longer be required. This hypothesis was originally minutes later midazolam was titrated to achieve a level
introduced by Moerman et al. [15]. Very few studies of moderate sedation (a patient who responds purpose-
have investigated use of remifentanil as a single agent for fully to verbal commands either alone or accompanied by
monitored anesthesia during colonoscopy [15, 16]. All light tactile stimulation). If the patient did not tolerate the
these studies have compared remifentanil with propofol. procedure, a supplemental dose of pethidine (25–75 mg
In our study we compared remifentanil with the sedative IV) and additional midazolam, up to a cumulative dose
combination most commonly used in colonoscopy, ben- of 0.1 mg kg–1 body weight was administered.
zodiazepines plus opioids [2]. Use of remifentanil (a Patients in group B (remifentanil) received, IV, a load-
relatively new l-opioid agonist) in endoscopic units ing dose of 1 lg kg–1 remifentanil over 60 s, by use of a
might have advantages over other drugs because of its medical pump, followed by continuous infusion at an initial
profound analgesic effects, rapid onset and offset time, rate of 0.05 lg kg–1 min–1, adjusted according to the
rapid titration to the individual patient’s requirements, analgesic end points insertion tolerance, no facial grimace
and no intermittent pain during colonoscopy [15, 16]. or complaint of pain, no movement.
Opiates are known to produce sedation and drowsiness Morbidity and mortality associated with colonoscopy
through l1 receptors [17]. were evaluated 30 days after the procedure.
This randomized prospective study was designed to
compare patient comfort, safety, recovery, and discharge
Monitoring and assessment of safety
after use of the opiate remifentanil compared with after
use of the standard combination of midazolam and
All patients were continuously monitored for heart rate
pethidine for moderate sedation. To the best of our
(HR) (three-lead electrocardiogram), oxygen saturation-
knowledge this is the first prospective randomized study
SpO2 (pulse oximetry), non-invasive mean arterial blood
in which remifentanil has been compared with the com-
pressure (MAP), and respiratory rate (RR) at 5-min
bination of midazolam plus pethidine during colonos-
intervals throughout the procedure. All patients were gi-
copy.
ven supplemental oxygen intranasally (2 L min–1).
Respiratory depression was considered significant ei-
ther when oxygen saturation was below 90% for more
Material and methods than 10 s on oxygen supplementation or when lack of
respiratory effort for more than 15 s was observed. A
Patient and control Subjects change in MAP or HR by 20% above or below the
baseline was considered significant. If a patient experi-
One-hundred and sixteen consecutive patients scheduled enced significant respiratory depression or deterioration
for complete colonoscopy participated in the study. All of consciousness which made verbal contact with the
colonoscopies were performed by the same experienced patient impossible, drug administration was stopped, jaw
endoscopist. thrust maneuver and bag mask ventilation were applied.
Sedation, analgesia, and monitoring were performed If these undesirable adverse events of respiratory
by the same qualified anesthesiologist. Patients were depression or deterioration of consciousness were not
randomly assigned to one of the two procedures by use resolved despite this intervention, the opioids reversal
of a table of random numbers. The study was not blind agent, naloxone, was administered.
for either the endoscopist or the anesthesiologist, because After completion of the colonoscopy patients were
of the obviously different appearances of the study transferred to the recovery area where MAP, HR, SpO2,
drugs. Associated medical illnesses were graded in RR, level of consciousness, APRS/MPADS scores, and
accordance with the American Society of Anesthesiolo- adverse effects such as nausea, vomiting, and pruritus were
gists’ Physical Status Classification (ASA grade) [18]. evaluated at 5-min intervals.
123
�36 Dig Dis Sci (2008) 53:34–40
Assessment of efficacy significant, a difference of 30 min in time to discharge,
with estimated standard deviation 40 to 50 min.
The extent of sedation was assessed by the anesthesiologist
by use of a sedation score (5 = not arousable, 4 = arous-
able to tactile stimulation, 3 = arousable to command, Results
2 = drowsy, 1 = awake) recorded every 5 min after drug
administration. Fifty-six patients were included in group A and sixty in
Recovery from sedation and hospital discharge were group B. Demographic data for the groups are listed in
assessed by use of the Modified Aldrete (APRS) [19] and Table 1.
the Discharge (MPADS) [20] scores, respectively. APRS The mean doses of midazolam and pethidine adminis-
and MPADS were evaluated every 5 min from removal of tered to members of group A were 4.1 ± 1 mg and
the endoscope until hospital discharge. The Aldrete and 83.1 ± 20.3 mg, respectively. The mean dose of remifenta-
Discharge scores are, respectively, established post-anes- nil administered to members of group B was 0.13 ±
thetic recovery and discharge scores. Aldrete takes into 0.08 lg kg–1 min–1.
account the color of the patient, respiration and circulation There was no difference between the two groups with
data, consciousness, and the patient’s activity. MPADS regard to duration of colonoscopy (Table 1).
takes into account the vital signs, ambulation and pain, and The numbers of significant drops in SpO2, MAP, and RR
side-effects such as nausea/vomiting and bleeding. The two were higher for group A than for group B. (Table 2). De-
scores range from 0–10. Ideally, the patient is fully spite this, cardiopulmonary complications did not occur
recovered and ready for discharge when these scores reach and there was no need for reversal agents or resuscitation in
10 points. either group.
Mean level of sedation was significantly higher in group
Patient assessment A than in group B (Table 2). During remifentanil admin-
istration all patients were mildly sedated, gave a lethargic
The quality of analgesia was assessed on the VAS scale response to verbal commands, and had mild ptosis of the
before hospital discharge [21]. The patient was asked to eyes. Although the target level of sedation in group A was
indicate the intensity of the pain experienced on the scale moderate sedation, most of those patients were moved to
with 0 being ‘‘no pain at all’’ and 10 ‘‘the worst pain deep sedation during the procedure.
imaginable’’. With regard to alterations in pain graded by the patients
The patient’s evaluation of the procedure (1 = unac- before discharge, no significant differences between the
ceptable, 2 = extremely uncomfortable, 3 = slightly two study groups were observed (Table 2).
uncomfortable, 4 = no discomfort) was obtained 24 h after Mean comfort level, as estimated by patients 24 h after
the procedure by telephone interview. The patients were the procedure, was no different for the two study groups
also asked whether or not they would prefer the same
sedation–analgesic medication should they need to undergo
a similar procedure in the future.
Table 1 Comparison of patients who received midazolam and
pethidine with those who received remifentanil
Endoscopist assessment
Group A Group B P value
Endoscopist satisfaction was assessed immediately after
Number (n) 56 60
the procedure as: 1, poor; 2, fair; 3, good; 4, excellent
Age (years)a 60.2 ± 11.5 60.3 ± 15.9 0.9
Gender 0.5
Statistical analysis
Male 34 33
Female 22 27
Continuous data were compared by use of the unpaired a
Weight (kg) 72.2 ± 11.3 74.6 ± 14.9 0.3
Student’s t test or the Mann–Whitney test, as appropriate.
Height (cm)a 164.6 ± 8.2 166.9 ± 8 0.1
Categorical variables were tested using corrected v2 or two
Duration (min)a 22.2 ± 2.9 23.1 ± 3.6 0.2
sided Fisher’s exact tests for univariate comparisons, as
ASA grade 0.3
appropriate. The criterion for statistical significance was
I 26 20
P < 0.05.
II 20 28
The sample size was calculated to achieve a statistical
power of 90% at 5% type I error. A sample size of III 10 12
a
60 patients was required for each group to detect, as Results are expressed as mean ± standard deviation
123
�Dig Dis Sci (2008) 53:34–40 37
Table 2 The efficacy and safety of sedation with midazolam and 100
pethidine compared with remifentanil Group
90
Group A, Group B, P value B
80
n = 56 n = 60
% of pa ti ent s di scha rge d
70 A
Drop in O2 saturation 10 1 P < 0.005
60
Drop in blood pressure 26 1 P < 0.001
Alteration in heart rate 2 8 P = 0.06 50
Drop in rate of respiration 16 0 P < 0.001 40
Mean sedation scorea 2.8 ± 0.4 1.4 ± 0.4 P < 0.001 30
a
Pain (VAS) 0.8 ± 1.5 1.15 ± 1.34 P = 0.2
20
Mean patient comfort levela 3.7 ± 0.5 3.7 ± 0.5 P = 0.7
10
Mean endoscopist comfort 3.6 ± 0.5 3.6 ± 0.5 P = 0.6
levela 0
APRS of 10 since completion 56 ± 11.3 0±0 P < 0.001 -10
of procedurea (min) 0 30 60 90 120 150 180 210 240 270 300
MPADS of 10 since completion 148.9 ± 34 28.7 ± 4.3 P < 0.001 Time (min)
of procedurea (min)
a
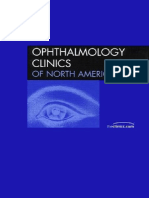
Results are expressed as mean ± standard deviation Fig. 1 Kaplan–Meier curve showing time to discharge (MPADS
score of 10)
(Table 2). The groups were equally satisfied with the
Discussion
medical procedures used and all members agreed to un-
dergo a later colonoscopy, if required, with the same
In this study safety and efficacy were compared and eval-
medication.
uated for remifentanil infusion and for the common com-
From the endoscopist’s point of view both groups
bination of midazolam and pethidine for moderate sedation
cooperated adequately with no statistical differences be-
during colonoscopy. The primary outcomes observed in
tween the two study groups (Table 2).
our study were shorter recovery and discharge times in the
Recovery (APRS of 10) was significantly sooner for
remifentanil group without affecting patient safety or sat-
the remifentanil group than for the midazolam + pethi-
isfaction. Benzodiazepines, opiates, and propofol in dif-
dine group (Table 2). Hospital discharge (MPADS of 10)
ferent combinations are commonly administered to provide
was significantly delayed for the midazolam + pethidine
conscious or deep sedation to patients undergoing painful
group compared with the remifentanil group (Table 2).
medical procedures such as colonoscopy [1–3, 7, 8, 10, 11,
Median discharge time for the midazolam + pethidine
13, 15, 16]. Unfortunately, all these procedures have side-
group was 165 min (95% confidence interval: 152–
effects and the objective of our efforts was to evaluate new
178 min), compared with less than 30 min for the rem-
sedation schemes to minimize these side-effects, to ensure
ifentanil group (95% confidence interval: 26–30 min). In
patient safety and convenience.
other words, median discharge time for the remifentanil
Remifentanil, a relatively new l-opioid receptor agonist
group was 5.5 times less than for the midazo-
has been successfully used as the analgesic component of
lam + pethidine group. As Fig. 1 clearly indicates, all
sedation techniques for regional and local anesthesia [22]
group B patients were discharged within 40 min whereas
and during colonoscopy [15, 16, 23, 24]. Remifentanil is
more than half of the group A patients were discharged
predominantly metabolized by nonspecific esterases, with
after two and a half hours. The earliest group A patient
extremely rapid clearance and offset of effect [25]. The
was discharged after 105 min.
context-sensitive half-life of remifentanil is consistently
There were no significant differences between post-
short, 3 to 5 min. Remifentanil also has a short effect–site
procedural adverse events in the two study groups. For
equilibration time of 1.0 to 1.5 min. This short equilibra-
three patients in group A and two patients in group B
tion time makes the onset of effect after drug administra-
discharge was delayed because of nausea and vomiting.
tion rapid, thus facilitating titration of the effect [25].
All patients were contacted by telephone 24 h and
Respiratory depression, a well known side-effect of
30 days after the procedure. No complications or deaths
opioids, is an expected adverse effect of remifentanil
associated with the colonoscopy were recorded during
administration. Respiratory depression is more frequently
the 30-day evaluation.
observed with rates of infusion above 0.2 lg kg–1 min–1
123
�38 Dig Dis Sci (2008) 53:34–40
[22]. The respiratory status of patients receiving remifen- Several studies have compared remifentanil and propo-
tanil must remain an important clinical and safety consid- fol infusion as adjuncts to local or regional anesthesia [22].
eration; when respiratory depression occurs, however, it is There have been very few studies of the use of remifentanil
resolved within approximately 3 min after remifentanil as a single agent in colonoscopy [15, 16]. Moerman et al.
dosing is reduced or stopped [22]. Published experience compared remifentanil and propofol for MAC during col-
with the use of remifentanil suggests it is possible to titrate onoscopy. In this study, remifentanil provided efficient
remifentanil administration to provide-effective analgesia pain relief, faster recovery of cognitive function, and
with minimum respiratory depression [22]. The problem of smoother hemodynamic profile than propofol when
remifentanil-induced respiratory depression is usually administered by trained professionals [15]. Moermam et al.
overcome in practice by cautious incremental titration of reported a significant difference in patient satisfac-
infusion to the desired effect, which should be analgesia tion—patient satisfaction was significantly higher in the
and comfort rather than sedation [22]. In our study patients propofol group than in the remifentanil group [15]. In our
did not experience significant respiratory depression, study, in contrast, there was no such difference. This dif-
probably because of careful titration of remifentanil infu- ference between the two studies might be explained by the
sion to patient comfort rather than sedation. Because different medication administered to the control group. In
remifentanil infusion requires 10 min to reach 95% of the study of Moerman et al. patients in the control group
steady-state concentration [25] and therefore adequate (propofol) were sedated to the level of deep sedation and
analgesic blood levels, we used a loading dose of 1 lg kg–1 they experienced very fast recovery time. In our study,
over 60 s beforehand to shorten the time until the patient however, the control patients (midazolam plus pethidine)
feels sufficiently comfortable to start the procedure. Bolus were sedated to the level of moderate sedation and their
doses of remifentanil must be administered slowly over recovery time was prolonged. Similarly to the study of
30–60 s to minimize the risk of respiratory depression [22]. Moerman et al., our study could be criticized for the dif-
The initial infusion rate in our study was chosen largely on ference between the level of sedation of the two groups.
the basis of previous studies which recommend an infusion Indeed, the drug in the remifentanil group was titrated
rate of 0.05–0.2 lg kg–1 min–1 when remifentanil is used according to patient comfort and safety rather than seda-
for monitored anesthesia care (MAC) or postoperative tion. In the study of Buvet et al. [16], remifentanil and
analgesia [15, 22, 26, 27]. In our study, we started with a propofol were used for patient-control analgesia (PCA)
relatively low infusion rate of remifentanil, 0.05 lg kg– during digestive endoscopic procedures [16]. The authors
1
min–1, titrated carefully to patient comfort with incre- concluded that self-administration of remifentanil is as
ments of 0.025 lg kg–1 min–1 to a maximum limit of effective as self administration of propofol. The PCA
0.2 lg kg–1 min–1, to minimize possible adverse events technique may not be the most efficient method of
[22]. We decided to change the current infusion rate rather administering sedation during endoscopy. The sedated
than administer bolus doses according to patient require- patients may have difficulties achieving appropriate use of
ments. This approach was based on current knowledge that PCA. If a steady state of remifentanil concentration in
bolus doses given concurrently with a continuous infusion blood is to be achieved, it is, moreover, more sensible to
of remifentanil increases the incidence of respiratory administer it as an infusion [25]. This mode of continuous
depression [22]. infusion was used in our study.
We decided to evaluate the benefits of using the short- In our study none of the remifentanil group patients
acting opiate remifentanil instead of the standard sedation experienced any cardiovascular instability or severe
scheme of midazolam and pethidine used in our depart- impairment in ventilation. Patients in group A, however,
ment, to test the hypothesis of Moerman et al. [15] that if experienced more side-effects including hypotension and
pain relief was adequate during colonoscopy sedation drops in RR and SpO2, than group B. The significant drops
would no longer be required. Studies in which a single in oxygen saturation and RR in this group of patients was
analgesic was used for colonoscopy in children had been probably because of synergistic interaction of the drugs,
reported during the previous decade [28]. The increasing which are known to cause clinically significant respiratory
pressure on endoscopic units to achieve shorter patient depression with hypoxia and even apnea [4, 5].
turn-around time, to enable more endoscopic procedures to The mean level of analgesia observed in our study
be conducted, has affected recent approaches to sedation. indicates that use of remifentanil is less beneficial than a
These efforts focus attention on alternative schemes instead combination of midazolam and pethidine; this is in
of the standard sedation scheme with midazolam and agreement with other studies [29]. This difference did not
pethidine. The primary objective of this study was to re- reach statistically significance in our study, however.
duce both recovery time and hospital discharge time after One explanation of this observation could be the lower
colonoscopy by using the short-acting opiate remifentanil. level of sedation in the remifentanil group than in the
123
�Dig Dis Sci (2008) 53:34–40 39
midazolam + pethidine group. All the patients in the 4. Bailey PL, Pace NL, Ashburn MA, Moll JW, East KA, Stanley
remifentanil group remained responsive during colonos- TH (1990) Frequent hypoxemia and apnea after sedation with
midazolam and fentanyl. Anesthesiology 73:826–830
copy, which was confirmed by the ability to communicate 5. Patel S, Vargo JJ, Khandwala F, Lopez R, Trolli P, Dumot JA,
with them at any time during the procedure. This did not Conwell DL, Zuccaro G (2005) Deep sedation occurs frequently
affect patient satisfaction. during elective endoscopy with meperidine and midazolam. Am J
Our results show that recovery and discharge was pro- Gastroenterol 100:2689–2695
6. Rex DK (2004) The science and politics of propofol. Am J
longed for the midazolam + pethidine group compared Gastroenterol 99:2080–2083
with the remifentanil group. Sedation is the major factor 7. Cohen LB, Dubovsky AN, Aisenberg J, Miller KM (2003)
keeping the patients waiting in the recovery area after Propofol for endoscopic sedation: A protocol for safe and
completing endoscopic procedures. The use of short-acting effective administration by the gastroenterologist. Gastrointest
Endosc 58:725–732
agents, for example remifentanil or propofol, reduces 8. Paspatis GA, Charoniti I, Manolaraki M, Vardas E, Papanikolaou
recovery time and, ultimately, the time in hospital, en- N, Anastasiadou A, Gritzali A (2006) Synergistic sedation with
abling shorter patient turn-around time in day case proce- oral midazolam as a premedication and intravenous propofol
dures. We would like to emphasize this observation, versus intravenous propofol alone in upper gastrointestinal en-
doscopies in children: a prospective, randomized study. J Pediatr
because there is a much interest in the literature regarding Gastroenterol Nutr 43:195–199
reduction of recovery time and time in hospital [1, 11]. 9. Koch ME, Gevirtz C (2004) Propofol may be safely administered
This is cost-saving for hospitals and probably important for by trained nonanesthesiologists. Con: Propofol: far from harm-
patient satisfaction. less. Am J Gastroenterol 99:1208–1211
10. Bell GD, Quine A (2006) Preparation, premedication, and sur-
Our study was approved by the Ethics Committee on the veillance. Endoscopy 38:105–109
understanding an anesthetist would be present in the 11. Lazzaroni M, Bianchi Porro G (2005) Preparation, premedica-
endoscopy suite. Use of an anesthetist to administer rem- tion, and surveillance. Endoscopy 37:101–109
ifentanil for colonoscopies limits its broader application, 12. Qadeer MA, Vargo JJ, Khandwala F, Lopez R, Zuccaro G (2005)
Propofol versus traditional sedative agents for gastrointestinal
because of the extra cost. If, however, such agents as endoscopy: a meta-analysis. Clin Gastroenterol Hepatol 3:1049–
remifentanil proved effective and safe in endoscopic 1056
sedation in large clinical trials, nurse-administered propo- 13. VanNatta ME, Rex DK (2006) Propofol alone titrated to deep
fol sedation might be considered. sedation versus propofol in combination with opioids and/or
benzodiazepines and titrated to moderate sedation for colonos-
In conclusion, our results suggest that use of remifen- copy. Am J Gastroenterol 101:2209–2217
tanil as a single agent during colonoscopy is associated 14. Cohen LB (2006) The future of endoscopic sedation. Proceedings
with faster patient recovery, and thus a shorter stay in of the 3rd annual endoscopic sedation meeting. New York,
hospital, than synergistic sedation with midazolam and pp 3–4
15. Moerman AT, Foubert LA, Herregods LL, Struys MM, De Wolf
pethidine, without affecting patient safety or satisfaction. DJ, De Looze DA, De Vos MM, Mortier EP (2003) Propofol
Our results also reinforce the hypothesis that if pain were versus remifentanil for monitored anaesthesia care during colo-
relieved adequately during colonoscopy sedation would no noscopy. Eur J Anaesthesiol 20:461–466
longer be required. Patients receiving remifentanil during 16. Bouvet L, Allaouchiche B, Duflo F, Debon R, Chassard D,
Boselli E (2004) Remifentanil is an effective alternative to
colonoscopy should, however, be aware, and accept that, propofol for patient-controlled analgesia during digestive endo-
they will probably be conscious during the examination. scopic procedures. Can J Anaesth 51:122–125
The safety profile of remifentanil was comparable to that of 17. Lauwers M, Camu F, Breivik H, Hagelberg A, Rosen M, Sneyd
synergistic sedation. These results should be confirmed in R, Horn A, Noronha D, Shaikh S (1999) The safety and effec-
tiveness of remifentanil as an adjunct sedative for regional
larger studies. anesthesia. Anesth Analg 88:134–140
18. Keats AS (1978) The ASA classification of physical status–a
recapitulation. Anesthesiology 49:233–236
References 19. Aldrete JA (1995) The post-anesthesia recovery score revisited. J
Clin Anesth 7:89–91
1. Rex DK (2006) Review article: moderate sedation for endoscopy: 20. Chung F, Chan VW, Ong D (1995) A post-anesthetic discharge
sedation regimens for non-anaesthesiologists. Aliment Pharmacol scoring system for home readiness after ambulatory surgery. J
Ther 24:163–171 Clin Anesth 7:500–506
2. Cohen LB, Wecsler JS, Gaetano JN, Benson AA, Miller KM, 21. Revill SI, Robinson JO, Rosen M, Hogg MI (1976) The reliability
Durkalski V, Aisenberg J (2006) Endoscopic sedation in the of a linear analogue for evaluating pain. Anaesthesia 31:1191–
United States: results from a nationwide survey. Am J Gastro- 1198
enterol 101:967–974 22. Servin F, Desmonts JM, Watkins WD (1999) Remifentanil as an
3. Paspatis GA, Manolaraki M, Xirouchakis G, Papanikolaou N, analgesic adjunct in local/regional anesthesia and in monitored
Chlouverakis G, Gritzali A (2002) Synergistic sedation with anesthesia care. Anesth Analg 89:S28–S32
midazolam and propofol versus midazolam and pethidine in 23. Rudner R, Jalowiecki P, Kawecki P, Gonciarz M, Mularczyk A,
colonoscopies: a prospective, randomized study. Am J Gastro- Petelenz M (2003) Conscious analgesia/sedation with remifen-
enterol 97:1963–1967 tanil and propofol versus total intravenous anesthesia with fen-
123
�40 Dig Dis Sci (2008) 53:34–40
tanyl, midazolam, and propofol for outpatient colonoscopy. remifentanil/midazolam for ambulatory surgery during monitored
Gastrointest Endosc 57:657–663 anesthesia care. Anesthesiology 87:51–57
24. Akcaboy ZN, Akcaboy EY, Albayrak D, Altinoren B, Dikmen B, 28. Bahal-O’Mara N, Nahata MC, Murray RD, Linscheid TR, Wil-
Gogus N (2006) Can remifentanil be a better choice than propofol liams T, Heitlinger LA, Li BU, McClung HJ, Lininger B (1993)
for colonoscopy during monitored anesthesia care? .Acta Ana- Efficacy of diazepam and meperidine in ambulatory pediatric
esthesiol Scand 50:736–741 patients undergoing endoscopy: a randomized, double-blind trial.
25. Glass PS, Gan TJ, Howell S (1999) A review of the pharmaco- J Pediatr Gastroenterol Nutr 16:387–392
kinetics and pharmacodynamics of remifentanil. Anesth Analg 29. Greilich PE, Virella CD, Rich JM, Kurada M, Roberts K, Warren
89:S7–S14 JF, Harford WV (2001) Remifentanil versus meperidine for
26. Avramov MN, Smith I, White PF (1996) Interactions between monitored anesthesia care: a comparison study in older patients
midazolam and remifentanil during monitored anesthesia care. undergoing ambulatory colonoscopy. Anesth Analg 92:80–84
Anesthesiology 85:1283–1289
27. Gold MI, Watkins WD, Sung YF, Yarmush J, Chung F, Uy NT,
Maurer W, Clarke MY, Jamerson BD (1997) Remifentanil versus
123