0% found this document useful (0 votes)
40 views1 pageSARS-CoV-2 Negative Test Certificate
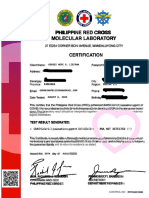
This document is a lab report certifying that a person tested negative for SARS-CoV-2. It provides the name of the tested individual, their passport or ID number, the date their specimen was collected, that a SARS-CoV-2 nucleic test was conducted, and that the results were negative. The report is signed and includes contact information for the certifying laboratory or health institution.
Uploaded by
Real Talk / Music '20Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
40 views1 pageSARS-CoV-2 Negative Test Certificate
This document is a lab report certifying that a person tested negative for SARS-CoV-2. It provides the name of the tested individual, their passport or ID number, the date their specimen was collected, that a SARS-CoV-2 nucleic test was conducted, and that the results were negative. The report is signed and includes contact information for the certifying laboratory or health institution.
Uploaded by
Real Talk / Music '20Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd