0% found this document useful (0 votes)
2K views18 pagesDaily Shift Report
The document defines a report as information about the existing situation that is exchanged between nurses to ensure continuity of care. A report includes a patient's medical history, medications, allergies, pain levels, and discharge instructions.
Good reports save time and prevent errors by providing full information about patient situations. Patients receive better care when reports contain all relevant data to prepare staff for the day's work. Reports can be oral, for immediate use, or written, for permanence and use by multiple people. Written reports should be clear, organized, and signed with identifying data. Daily reports include details on admissions, discharges, transfers, deaths, procedures, IVs, tubes, dressings, and patients requiring observation or off-
Uploaded by
Alaa HamoudaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
2K views18 pagesDaily Shift Report
The document defines a report as information about the existing situation that is exchanged between nurses to ensure continuity of care. A report includes a patient's medical history, medications, allergies, pain levels, and discharge instructions.
Good reports save time and prevent errors by providing full information about patient situations. Patients receive better care when reports contain all relevant data to prepare staff for the day's work. Reports can be oral, for immediate use, or written, for permanence and use by multiple people. Written reports should be clear, organized, and signed with identifying data. Daily reports include details on admissions, discharges, transfers, deaths, procedures, IVs, tubes, dressings, and patients requiring observation or off-
Uploaded by
Alaa HamoudaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
- Daily Shift Report Overview: Introduces the daily shift report detailing orientation, purpose, and the importance for continuity of care and clinical practices.
- Importance of Shift Report: Discusses the benefits and necessity of maintaining comprehensive and accurate shift reports for ensuring seamless patient care.
- Types and Characteristics of Shift Reports: Explains the two major shift report types: Oral and Written, including their characteristics, usage contexts, and presentation standards.
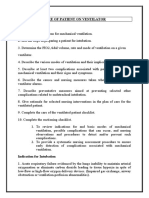
- Contents Required in a Daily Shift Report: Details specific case types and the critical information to include for each in daily shift reports to ensure comprehensive patient tracking.
- Application of Daily Shift Report: Provides an example scenario demonstrating the use of shift reports in surgical departments, highlighting patient notes and observations.
- Shift Report Example: Shows a completed daily shift report form example, illustrating the standard layout and expected detail level.
- Conclusion: Concludes the document with a note of appreciation and final thoughts.