100% found this document useful (1 vote)
468 views2 pagesGF3 Individual Inventory Record Form
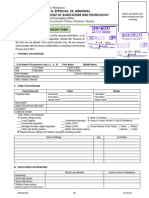
This document is an individual inventory form used by Bohol Island State University to gather personal information about students. The form collects details such as the student's name, age, contact information, family background, educational history, interests, talents, concerns, and health information. It is intended to help guidance counselors provide support and assistance to students. Completing the form ensures counselors have essential data that enables them to aid students in a confidential manner.
Uploaded by
Aira Mae PustaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
100% found this document useful (1 vote)
468 views2 pagesGF3 Individual Inventory Record Form
This document is an individual inventory form used by Bohol Island State University to gather personal information about students. The form collects details such as the student's name, age, contact information, family background, educational history, interests, talents, concerns, and health information. It is intended to help guidance counselors provide support and assistance to students. Completing the form ensures counselors have essential data that enables them to aid students in a confidential manner.
Uploaded by
Aira Mae PustaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd