0% found this document useful (0 votes)
1K views1 pageImaging Request Form
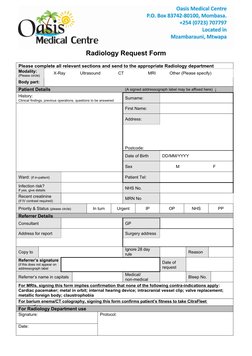
The radiology request form collects essential patient information such as name, date of birth, contact details, medical history, and type of imaging exam requested. It also requires information on the referring clinician and their signature. The form is used to schedule and prioritize imaging exams and ensure patient safety for procedures requiring contrast or bowel preparation.
Uploaded by
elmore kakaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
1K views1 pageImaging Request Form
The radiology request form collects essential patient information such as name, date of birth, contact details, medical history, and type of imaging exam requested. It also requires information on the referring clinician and their signature. The form is used to schedule and prioritize imaging exams and ensure patient safety for procedures requiring contrast or bowel preparation.
Uploaded by
elmore kakaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd
- Radiology Request Form: This page contains a Radiology Request Form for the Oasis Medical Centre, including sections for patient details, referring doctor's information, and required scans.