Gil 2012
Uploaded by
niriGil 2012
Uploaded by
niriSPECIAL ISSUE PAPER
First Anxiety, Afterwards Depression: Psychological
Distress in Cancer Patients at Diagnosis and after
Medical Treatment
Francisco Gil1*†, Gema Costa2, Ines Hilker1 & Llucia Benito3
1
Psycho-oncology Unit, Duran i Reynals Hospital, Institut Català d’Oncologia, L’Hospitalet de Llobregat, Barcelona, Spain
2
Department of Psychiatry, Hospital de Mataró, Mataró, Barcelona, Spain
3
Control and Preventive Service, Duran i Reynals Hospital, Institut Català d’Oncologia, L’Hospitalet de Llobregat, Barcelona, Spain
Abstract
Objective: The purpose of this study was to assess psychosocial changes at two particular moments: at cancer
diagnosis and 2–4 weeks after having finished treatment.
Material and methods: A total of 67 cancer outpatients were assessed in this study. The inclusion/exclusion criteria
were as follows: ambulatory cancer patients aged 18 years or older and receiving medical treatment. Patients with a
performance status <50 or with cognitive impairment (≥3 errors in the Pfeiffer Questionnaire) were excluded. The
inclusion period ranged from 1 April 2005 to 30 April 2007. The scales used were the 14-item Hospital Anxiety and
Depression Scale (HADS), which has two subscales for anxiety (seven items) and for depression (seven items), the Quality
of Life Short Form 36 Questionnaire, the Mental Adjustment Scale and the Medical Outcomes Study Questionnaire for
measuring social support. All data were compared with sociodemographic and medical characteristics.
Results: Patients had higher levels of pre-treatment versus post-treatment anxiety (HADS-Anxiety mean, 7.41 versus 6.69),
whereas depression scores were higher post-treatment versus pre-treatment (HADS-Depression mean, 3.14 versus 3.89).
After medical treatment, patients were more fatigued, with lower performance status (Karnofsky Index), less social
support and less quality of life, but no differences in coping styles were found. Women had higher levels of anxiety
than men. Patients with psychiatric antecedents had higher levels of distress, but these differences were only observed
after diagnosis and not after the treatment. In general, head and neck cancer patients had higher levels of distress, worse
coping and worse social functioning.
Conclusions: Cancer patients require special consideration before and after treatment. Anxiety is the symptom that
characterizes diagnosis, whereas depression is more common after medical treatment. The head and neck cancer
patients were the group with the highest complexity. Copyright © 2012 John Wiley & Sons, Ltd.
Received 8 February 2012; Accepted 20 July 2012; Revised 14 June 2012
Keywords
cancer; distress; quality of life; coping; social support
*Correspondence
Francisco Gil, Psycho-oncology Unit, Duran i Reynals Hospital, Institut Català d’Oncologia, L’Hospitalet de Llobregat, Barcelona, Spain.
†
E-mail: fgil@iconcologia.net
This study received ethical approval from the Ethics Board of the Hospital Universitario de Bellvitge, L’Hospitalet, Barcelona, Spain.
Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/smi.2445
Introduction Approximately one in four cancer patients is diag-
The diagnosis of cancer is accompanied by a sense of nosed with a psychiatric disorder (Brintzenhofe-Szoc,
threat and incertitude about your life. After diagnosis, Levin, Li, Kissane, & Zabora, 2009; Bultz et al., 2011),
fear of suffering and death produces feelings of anxiety and a significant proportion of cancer patients at all
(Akechi, Nakano, Akizuki et al., 2002; Alonso, Prieto, stages of disease will suffer emotional and psychological
& Antón, 1995; Annunziata, Muzzati, & Bidoli, 2010). morbidity as a result of diagnosis and treatment
And after ending cancer treatment, fear of recurrence may (Colmes, 2001; Brintzenhofe-Szoc et al., 2009). In a
evoke feelings of depression in metastatic gastrointestinal landmark study by Derogatis et al., 47% (101 of 215
and lung cancer patients (Boyes, Girgis, D’Este, & patients) of cancer patients presented some type of
Zucca, 2011). mental disorder, the most common being psychological
Stress Health (2012)© 2012 John Wiley & Sons, Ltd.
First Anxiety, Afterwards Depression F. Gil et al.
adjustment disorders (anxiety and/or depressive mood; (1) The Hospital Anxiety and Depression Scale
68%) and clinical depression (13%) (Costa, Salamero, (HADS; Grassi et al., 2004) assesses psychological
& Gil, 2007). A study with 277 cancer patients in Italy, distress, which is a 14-item questionnaire with
Portugal and Spain reported that 28.5% of these patients two subscales (seven items each) for anxiety and
were defined as clinical cases requiring psychological depression symptoms. Each item is rated on a
care (Costa & Gil, 2009a). Likewise, cancer patients have four-point Likert scale from 0 to 3.
a higher risk of suicide than the general population. (2) The Medical Outcomes Study Social Support
Akechi et al. found that 62 of 1713 cancer patients Survey (MOS-SSS; Hill et al., 2011) assesses
(4%) referred for psychiatric treatment had some form the multidimensionality of perception of social
of suicidal behaviour, generally associated with depres- support in cancer patients. It has 20 items, with
sion and low performance status (Costa & Gil, 2009b). four domains: emotional/informational support,
Likewise, low social support is a predictor of depression affective support, interaction support and instru-
and anxiety disorder (Derogatis, Morrow, Fetting et al., mental support. In each domain, except for item
1983). These data show the necessity of integrating 1, the MOS-SSS scale scores range from 1 (never)
screening for distress in routine care (Gil, Costa, & to 5 (always). A high score represents a high
Pérez, 2010; Gil et al., 2008). However, only a small num- perception of social support. Item 1 assesses qual-
ber of oncologists use standardized measure of distress itative support (e.g. number of close friends or
(smi2445-bib-0012Gil, Grassi, Travado, Tomamichel, & relatives). We can obtain a global index of social
González, 2005; smi2445-bib-0013Gil, Grassi, Travado, support with the sum of the other 19 items.
Tomamichel, & Gonzalez, 2005). (3) The Mental Adjustment Scale (Hinz et al., 2009)
Distress has been defined by the National Comprehen- is used to assess the cognitive responses to a
sive Cancer Network as an unpleasant experience of cancer diagnosis. It is a 40-item self-rating
a psychological, social and/or spiritual nature, which questionnaire that uses a four-point Likert scale,
extends on a continuum from normal feelings of which includes the following five behavioural
vulnerability, sadness and fears to disabling problems styles: fighting spirit (16 items) is when patients
such as depression, anxiety, social isolation and spiritual fully accept the diagnosis, characterized by the
crisis, branding distress as the sixth vital sign in cancer care, adoption of an optimistic attitude; helpless–
after being considered as vital signs body temperature, hopeless (six items) is characterized by feelings
pulse (or heart rate), blood pressure, respiratory rate and of giving up and engulfment by knowledge of
pain (Gil et al., 2005, 2005). the diagnosis; anxious pre-occupation (nine items)
The purpose of this study was to assess psychosocial is characterized by constant pre-occupation with
changes at two specific moments: upon cancer diagnosis cancer and feelings of threat; fatalism (eight items)
and at 2–4 weeks post-treatment. shows an attitude of resigned, passive acceptance
of the cancer; and avoidance (denial; one item)
Methods is when patients avoid the word ‘cancer’ by using
various euphemisms.
Sample/participants (4) The Medical Outcome Study Short Form-36
The study sample consisted of 67 ambulatory cancer (MOS SF-36; Holland & Bultz, 2007) provides a
patients aged 18 years or older who were receiving medical general measure of health-related quality of life
treatment at the Hospital Duran i Reynals, Catalan in eight domains: physical functioning, limitations
Institute of Cancer, L’Hospitalet, Barcelona, Spain. in performing roles because of physical health
problems (physical roles), bodily pain, general
health, vitality, social functioning, limitations in
Procedure performing roles due to emotional health pro-
All patients who agreed to participate in the study were blems (emotional roles) and mental health. In
assessed by a clinical psychologist during the disease each domain, MOS SF-36 scale scores range from 0
trajectory: after diagnosis (pre-treatment) and before (the worst possible measured health) to 100 (the
medical treatment (surgery, chemotherapy or radio- best possible measured health) with higher scores
therapy) and 2–4 weeks after having finished medical representing better functioning. The questionnaire
treatment. The role of the clinical psychologist was only also provides two general health domains: physical
to explain the purpose of the study to patients and to health and mental health. The MOS SF-36
distribute the questionnaires; no psychological support has been translated and adapted into Spanish
services were offered. Once the informed consent form and has shown satisfactory reliability and valid-
was signed, several different psychological measures ity (Holmes, 2008; Ibbotson, Maguire, Selby,
were used to assess the possible changes at two specific Priestman, & Wallace, 1994).
moments: upon cancer diagnosis and 2–4 weeks post-
treatment. The questionnaires described as follows were In addition to the psychological measures described
completed at one of our outpatient consultations: earlier, we also collected data on the following:
Stress Health (2012)© 2012 John Wiley & Sons, Ltd.
F. Gil et al. First Anxiety, Afterwards Depression
(5) Symptoms: pain, anorexia, constipation, insomnia, scores were higher (mean score, 7.41) than the cut-off
tiredness and dry mouth. All patients were level of 7; for post-treatment, only 56% of the patients
asked about the presence and the intensity of remained above the cut-off level, with a mean anxiety
these six physical symptoms, with intensity
recorded on a scale from 0 (minimum) to 10 score of 6.69, a non-significant difference (p = 0.14).
(maximum). All scores above 7 are considered possible clinical
(6) Pfeiffer Questionnaire: used to detect cognitive cases. Pre-treatment and post-treatment scores on the
deficit. The cut-off score is ≥3 errors (Inen, HADS-Depression (mean, 3.14 versus 3.89, respectively;
Ranchor, Sanderman et al., 2008). p = 0.05) indicated that depression scores worsened after
(7) Karnofsky performance status: this scale treatment, with 22% of the patients above the cut-off
assesses functional capacity. It has a range from level of 7 after treatment versus only 12% before. The
100 (intact functional capacity) to 0 (death) total HADS score was similar before and after cancer
(Karnofsky & Burchenal, 1949). treatment [mean, 10.56 (29% of the patients above the
(8) Medical and sociodemographic characteristics cut-off) versus 10.58 (29%); p = 0.97; Table II; Figure 1].
of patients.
After treatment, patients with head and neck cancer
were more distressed (HADS-Total) than other group
Statistical analysis of patients (head and neck cancer, 14.78; breast cancer,
The SPSS version 17.0 (SPSS, Inc., Chicago, IL, USA) 8.88; colorectal cancer, 10; p = 0.05). In terms of coping
was used for statistical analyses. First, we used a scores, head and neck cancer patients had higher levels
descriptive univariate analysis with all the variables of of anxious pre-occupation than other patients (head
the study. After the first analysis, we used an analysis and neck cancer, 23.42; breast cancer, 22.49; colorectal
of variance of a factor for repeated measures. In our cancer, 19.91; p = 0.05).
case, the factor was the time, with two different
moments: the first moment was after diagnosis and Quality of life
before starting cancer treatment (time 1), and the The level of quality of life after treatment is lower than
second moment was during the follow-up (2–4 weeks before treatment. After treatment, as physical function-
after having ended cancer treatment; time 2). ing is worse than before (mean, 80.36 versus 74.90;
p = 0.03), more limitations in performing roles were
Results observed, because of physical health problems (mean,
57.60 versus 37.19; p = 0.00), more bodily pain (mean,
Subjects
70.83 versus 58.90; p = 0.00), less vitality (mean, 68.86
Of the 92 cancer patients invited to participate in the versus 50.90; p = 0.00) and worse social functioning
study, 25 refused to participate owing to emotional dif- (mean, 83.33 versus 70.83, p = 0.00). Patients with
ficulties in talking about the illness, physical symptoms psychiatric history had lower levels of vitality (mean,
or lack of time. The median time between diagnosis 53.75 versus 73.59; p = 0.00). No differences in quality
and the clinical interview was 6 months (range, 12 days of life were observed between the patients when
to 190 months). Forty-two were women, with a mean considering cancer diagnosis.
age of 52 years, 85% married, 51% with high school
level or higher, 91% had at least a child, 61% had rela- Social support
tives with cancer and 40% had relatives died of cancer. In general, patients received less social support after
Twenty-two per cent had previous psychiatry history, cancer treatment (mean, 87.46 versus 83.52; p = 0.00).
and 36% had previous familial psychiatric history. In particular, patients had less emotional (mean,
Fifty-four percent had breast cancer, 25% had head 36.19 versus 34.11; p = 0.00), instrumental (mean,
and neck cancer, 19% had colorectal cancer, and 2% 18.70 versus 17.87; p = 0.01) and affective support
had digestive cancer. Ninety-nine percent of them (mean, 14.42 versus 13.89; p = 0.01) after treatment
had a local or loco-regional illness (Table I). (Table II). Men (mean, 61.87 versus 76.10; p = 0.04)
There were no errors in the Pfeiffer Questionnaire, and head and neck cancer patients had less social func-
and patients had good performance status (Karnofsky tioning compared with other patients (head and neck
Index) before and after cancer treatment but with more cancer, 51.13; breast cancer, 75.59; colorectal cancer,
fatigue after the treatment (Table II). 78.12; p = 0.02). Women perceived less social support
(instrumental support) than men (mean, 16.40 versus
Psychological distress and coping 19.26; p = 0.00) after medical treatment.
Women were more anxious than men after the diagnosis
(mean, 8.16 versus 6.16; p = 0.05). But less helpless– Discussion
hopeless (mean, 7.57 versus 9.04; p = 0.05). The presence Cancer patients are more anxious at diagnosis and
of psychiatric history increases the level of distress but more depressed after cancer treatment. The higher
only after the diagnosis and not after ending medical levels of anxiety at the start of cancer treatment may
treatment (mean, 14.53 versus 9.41; p = 0.00). In 46 of profit from mental health support (Lo, Zimmermann,
the 67 patients evaluated (69%), pre-treatment anxiety Rydall et al., 2010; Martinez de la Iglesia, Dueñas, Onis
Stress Health (2012)© 2012 John Wiley & Sons, Ltd.
First Anxiety, Afterwards Depression F. Gil et al.
Table I. Sociodemographic and medical characteristics
Demographics (N= 67)
Age (years) Mean: 52 years Standard deviation: 10.64
Sex Men 25 37%
Women 42 63%
Civil status Married 57 85%
Divorced 5 8%
Single 4 6%
Widowed 1 1%
Educational level Less than high school 33 49%
High school 29 43%
University 5 8%
Children 0 6 9%
1 18 27%
2 30 45%
3 9 13%
4 4 6%
Relatives with cancer Yes 41 61%
No 26 39%
Relatives died of cancer Yes 27 40%
No 40 60%
Personal psychiatric history Yes 15 22%
No 52 78%
Familial psychiatric history Yes 24 36%
No 43 64%
Cancer diagnosis Breast 36 54%
Head and neck 17 25%
Colorectal 13 19%
Digestive 1 2%
Cancer status Local 44 66%
Locoregional 22 33%
Advanced 1 1%
Type of treatment Surgery 55 82%
Radiotherapy 30 45%
Chemotherapy 27 41%
et al., 2001). Several studies have established the sensitivity, by patients and their relatives, once ended chemotherapy
specificity and optimal cut-off scores of some measures, as and radiotherapy treatments, that they do not want to wait
the distress thermometer (DT) and the HADS. Cut-off 3 or 4 months until the next visit with their doctor. They
scores of 4 on the DT and 10 for the HADS have indicated feel that the follow-up is too far away, and they need to
acceptable sensitivity and specificity to detect a current be in contact with their doctor. We find support for this
psychiatric disorder (Patel, Sharpe, Thewes, Bell, & Clarke, idea in a previous study in which we observed that chemo-
2011; Pirl, Muriel, Hwang et al., 2007). The emotional therapy treatment reduced the level of emotional distress
impact after notifying the presence of cancer can explain (Bultz et al., 2011).
the higher levels of distress at diagnosis. However, once Other possible explanation is the presence of phys-
ended the cancer treatment, patients are more aware about ical symptoms, once ended the treatments. Fatigue
the meaning of a cancer diagnosis in their life, and we can and pain are associated with higher levels of anxiety
observe a growing awareness of the impact of the illness on and depression symptoms during the follow-up
all domains of life, feeling more depressed (Boyes et al., (Schwarz, Krauss, Höckel et al., 2008). Likewise, the
2011). Another possible explanation receives support lower level of quality of life and the less social support
by the secure base literature (Razavi & Delvaux, 1995; received after cancer treatment can increase the level
Stanton, Ganz, Rowland et al., 2005). The patient can see of emotional distress. The prevalence of high levels of
his or her oncologist as his or her secure base; but the psychosocial morbidity after ending cancer treatments
frequency of medical contact decreases during the surveil- emphasizes the need for routine psychosocial assessment
lance phase of treatment, and he or she can begin to worry throughout the cancer trajectory (Vahdaninia, Omidvari,
more about recurrence. It is very common to be informed & Montazeri, 2010).
Stress Health (2012)© 2012 John Wiley & Sons, Ltd.
F. Gil et al. First Anxiety, Afterwards Depression
Table II. Medical and psychological characteristics before and after the cancer treatment
Before (mean and SD) After (mean and SD) p
Symptoms Pain 2.71 (0.87) 3.44 (0.85) >0.05
Anorexia 1.44 (0.71) 1.23 (0.72) >0.05
Constipation 1.69 (0.81) 1.75 (0.79) >0.05
Insomnia 2.34 (0.82) 2.59 (0.88) >0.05
Fatigue 2.65 (0.85) 5.26 (0.75) <0.05
Dry mouth 2.19 (0.75) 3.69 (1.00) >0.05
Karnofsky Index 83.46 (9.01) 80.76 (7.36) <0.05
Pfeiffer Index No errors (intact) No errors (intact) >0.05
HADS Anxiety 7.41 (4.11) 6.69 (3.81) 0.14
Depression 3.14 (3.16) 3.89 (3.55) 0.05
Total 10.56 (6.68) 10.58 (6.83) 0.97
MAC Fighting spirit 51.79 (6.09) 50.47 (7.44) 0.13
Helpless–hopeless 7.64 (2.37) 8.12 (3.05) 0.21
Anxious pre-occupation 22.33 (5.10) 21.86 (4.11) 0.42
Fatalism 21.48 (4.73) 21.50 (5.07) 0.97
Avoidance 1.52 (0.92) 1.45 (0.70) 0.56
MOS Emotional/informational support 36.19 (4.46) 34.11 (6.28) 0.00
Instrumental support 18.70 (2.12) 17.87 (2.88) 0.01
Interactional support 18.14 (2.58) 17.63 (2.68) 0.12
Affective support 14.42 (1.18) 13.89 (1.82) 0.01
Total support 87.46 (9.14) 83.52 (12.42) 0.00
SF-36 Physical functioning 80.36 (21.89) 74.90 (16.92) 0.03
Physical roles 57.60 (34.87) 37.19 (24.48) 0.00
Bodily pain 70.83 (26.90) 58.90 (27.41) 0.00
General health 66.69 (20.18) 63.56 (19.65) 0.19
Vitality 68.86 (21.66) 50.90 (22.89) 0.00
Social functioning 83.33 (24.52) 70.83 (25.46) 0.00
Emotional roles 89.35 (22.62) 84.72 (21.76) 0.14
Mental health 67.54 (20.56) 70.27 (22.71) 0.30
SD: standard deviation; HADS: Hospital Anxiety and Depression Scale; MAC: Mental Adjustment Scale; MOS: Medical Outcomes Study; SF-36:
Short Form.
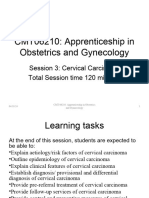
HADS Total
HADS Anxiety
HADS Depression
Limitations
This study has several limitations. The first limitation is
15
the small sample size (67 patients). Another limitation
is that the results are only applicable to certain cancer
localizations (breast, head and neck, colorectal and
10 digestive). And finally, we only evaluated patients with
local or locoregional cancer status, with only a few
cases of metastatic cancer.
5
Conclusion
We found that anxiety and depressive symptoms are
common both before and after treatment for cancer.
Diagnosis After ending the treatment The increase in depression following treatment was
remarkable and merits further attention. It seems clear
Figure 1 Hospital Anxiety and Depression Scale scores in the diag- that physicians need to pay particular attention to the
nosis and after the cancer treatment patient’s psychological status not only before treatment
but also afterwards to refer at-risk patients to psycho-
Head and neck cancer patients present more com- oncology services for treatment. Future research is
plexity and worse psychological adjustment. Stomach needed to assess the reasons for these high levels of
cancer, pancreatic cancer, lung cancer and head and neck anxiety and depression symptoms before and after
cancer have higher levels of mixed anxiety/depression treatment, particularly post-treatment, which was the
symptoms (Ware & Sherbourne, 1992). most surprising finding in our study.
Stress Health (2012)© 2012 John Wiley & Sons, Ltd.
First Anxiety, Afterwards Depression F. Gil et al.
Acknowledgments gratitude to these cancer patients who kindly
This research was supported by a grant from volunteered to participate in this study. We wish
the Agency of Technology Evaluation and Medical to thank Bradley Londres for his assistance in editing
Research (AATRM 102/19/2004). We express our the text.
Gil, F., Grassi, L., Travado, L., Tomamichel, M., & distress in breast cancer patients, their partners, and
REFERENCES González, J.R. (2005a). Use of distress and depression matched control couples. Annals of Behavioral
Akechi, T., Nakano, T., Akizuki, N., Nakanishi, T., thermometers to measure psychosocial morbidity Medicine, 36, 141–148.
Yoshikawa, E., Okamura, H., & Uchitomi, Y. among Southern European cancer patients. Supportive Karnofsky, D.A., & Burchenal, J.H. (1949). The clinical
(2002). Clinical factors associated with suicidality in Care in Cancer, 13(8), 600–606. evaluation of chemotherapeutic agents in cancer. In
cancer patients. Japanese Journal of Clinical Oncology, Gil, F., Grassi, L., Travado, L., Tomamichel, M., & C.M. MacLeod (Ed.), Evaluation of Chemotherapeutic
32(12), 506–511. Gonzalez, J.R. (2005b). Use of distress and depression Agents (pp. 191–205). New York: Columbia University
Alonso, J., Prieto, L., & Antón, J.M. (1995). La versión thermometers to measure psychosocial morbidity Press.
española del SF-36 Health Survey (Cuestionario de among southern European cancer patients. Supportive Lo, C., Zimmermann, C., Rydall, A., Walsh, A.,
Salud SF-36): un instrumento para la medida de los Care in Cancer, 13, 600–606. Jones, J.M., Moore, M.J., . . . Rodin, G. (2010).
resultados. Medicina Clinica, 104, 771–776. Gil, F., Costa, G., & Pérez, F.J. (2010). Does chemother- Longitudinal study of depressive symptoms in
Annunziata, M.A., Muzzati, B., & Bidoli, E. (2010). apy reduce stress? Palliative and Supportive Care, 8, patients with metastatic gastrointestinal and lung
Psychological distress and needs of cancer patients: 455–460. cancer. Journal of Clinical Oncology, 28, 3084–3089.
A prospective comparison between the diagnostic Gil, F., Costa, G., Pérez, F.J., Salamero, M., Sánchez, N., Martinez de la Iglesia, J., Dueñas, R., Onis, M.C.,
and therapeutic phase. Supportive Care in Cancer, 19(2), & Sirgo, A. (2008). Adaptación psicológica y preva- Aguado, C., Albert, C., & Luque, R. (2001). Adapta-
291–295. lencia de trastornos mentales en pacientes con cáncer ción y validación al castellano del cuestionario de
Boyes, A.W., Girgis, A., D´Este, C., & Zucca, A.C. (Psychological adaptation and prevalence of mental Pfeiffer (SPMSQ) para detectar la existencia de
(2011). Flourishing or floundering? Prevalence disorders in cancer patients). Medicina Clínica, 130(3), deterioro cognitivo en personas mayores de 65 años
and correlates of anxiety and depression among a 90–92. (Adaptation and validation to Spanish of the Pfeiffer
population-based sample of adult cancer survivors Grassi, L., Travado, L., Gil, F., Sabato, S., Rossi, E., & questionnaire (SPMSQ) for detecting cognitive defi-
6 months after diagnosis. Journal of Affective Disorders, The SEPOS Group. (2004). Psychosocial morbidity cit in adults older than 65 years. Medicina Clínica,
135(1–3), 184–192. and its correlates in cancer patients of the Mediterra- 117, 129–134.
Brintzenhofe-Szoc, K.M., Levin, T.T., Li, Y., Kissane, D.W., nean area: Findings from the Southern European Patel, D., Sharpe, L., Thewes, B., Bell, M.L., & Clarke, S.
& Zabora, J.R. (2009). Mixed anxiety/depression Psycho-Oncology Study. Journal of Affective Disorders, (2011). Using the distress thermometer and Hospital
symptoms in a large cancer cohort: Prevalence by 83, 243–248. Anxiety and Depression Scale to screen for psychosocial
cancer type. Psychosomatics: Journal of Consultation Hill, J.J., Hokombe, C.C., Clark, L.L., Boothby, M., morbidity in patients diagnosed with colorectal cancer.
Liaison Psychiatry, 50(4), 383–391. Hincks, A.A., Fisher, J.J., & Salmon, P.P. (2011). Journal of Affective Disorders, 131(1–3), 412–416.
Bultz, B.D., Groff, S.L., Fitch, M., Blais, M.C., Howes, Predictors of onset of depression and anxiety in the Pirl, W.F., Muriel, A., Hwang, V., Kornblith, A., Greer, J.,
J., Levy, K., & Mayer, C. (2011). Implementing year after diagnosis of breast cancer. Psychological Donelan, K., . . . Schapira, L. (2007). Screening for
screening for distress, the 6th vital sign: A Canadian Medicine: A Journal of Research in Psychiatry and the psychosocial distress: A national survey of oncologists.
strategy for changing practice. Psycho-Oncology, 20, Allied Sciences, 41(7), 1429–1436. The Journal of Supportive Oncology, 5(10), 499–504.
463–469. Hinz, A., Krauss, O., Stolzenburg, J.-U., Schwalenberg, Razavi, D., & Delvaux, N. (1995). The psychiatrist’s
Colmes, J. (2001). The Search for the Secure Base. New T., Michalski, D., & Schwarz, R. (2009). Anxiety perspective on quality of life and quality of care in
Cork: Routledge. and depression in patients with prostate cancer and oncology: Concepts, symptom management, and
Costa, G., & Gil, F.. (2009a). The mental adjustment other urogenital cancer: A longitudinal study. Uro- communication issues. European Journal of Cancer
to cancer scale: A psychometric analysis in Spanish logic Oncology: Seminars and Original Investigations, 31A Suppl. 6, S25–29.
cancer patients. Psycho-Oncology, 18, 984–991. 27(4), 367–372. Schwarz, R., Krauss, O., Höckel, M., Meyer, A., Zenger,
Costa, G., & Gil, F. (2009b). Quality of life in the Holland, J.C., & Bultz, B.D. (2007). National Compre- M., & Hinz, A. (2008). The course of anxiety and de-
chemotherapy treatment of Spanish cancer patients: A hensive Cancer Network (NCCN). The NCCN pression in patients with breast cancer and gynaeco-
comparison of general population. Psycho-Oncology, guideline for distress management: A case for making logical cancer. Breast Care, 3, 417–422.
18, 1053–1059. distress the sixth vital sign. Journal of the National Stanton, A.L., Ganz, P.A., Rowland, J.H., Meyerowitz,
Costa, G., Salamero, M., & Gil, F. (2007). Validación del Comprehensive Cancer Network, 5(1), 3–7. B.E., Krupnick, J.L., & Sears, S.R. (2005). Promoting
cuestionario MOS-SSS de apoyo social en pacientes Holmes, J. (2008). The Search for the Secure Base: adjustment alter treatment for cancer. Cancer, 104
con cáncer (Validity of the questionnaire MOS-SSS Attachment Theory and Psychotherapy. New York: (suppl 11), 2608–2613.
of social support in neoplastic patients). Medicina Routledge. Vahdaninia, M., Omidvari, S., & Montazeri, A. (2010).
Clínica, 128(18), 687–691. Ibbotson, T., Maguire, P., Selby, P., Priestman, T., & What do predict anxiety and depression in breast
Derogatis, L.R., Morrow, G.R., Fetting, J., Penman, D., Wallace, L. (1994). Screening for anxiety and depres- cancer patients? A follow-up study. Social Psychiatry
Piasetsky, S., Schmale, A.M., . . . Carnicke, C.L. Jr. sion in cancer patients: The effects of disease and and Psychiatric Epidemiology, 45(3), 355–361.
(1983). The prevalence of psychiatric disorders treatment. European Journal of Cancer, 30, 37–40. Ware, J.R., & Sherbourne, C.D. (1992). The MOS
among cancer patients. JAMA: The Journal of the Hinnen, C., Ranchor, A.V., Sanderman, R., Snijders, T., 36-item Short-Form Health Survey (SF-36). Medical
American Medical Association, 249, 751–757. Hagedoorn, M., & Coyne, J.C. (2008). Course of Care, 30(6), 473–481.
Stress Health (2012)© 2012 John Wiley & Sons, Ltd.
You might also like
- Psycho Oncology 150131012138 Conversion Gate01No ratings yetPsycho Oncology 150131012138 Conversion Gate0194 pages
- Depression and Anxiety in Cancer PatientsNo ratings yetDepression and Anxiety in Cancer Patients34 pages
- Oncology Patients' Anxiety & Depression StudyNo ratings yetOncology Patients' Anxiety & Depression Study4 pages
- New Research in Psychooncology: Current Opinion in Psychiatry April 2008No ratings yetNew Research in Psychooncology: Current Opinion in Psychiatry April 20086 pages
- New Research in Psychooncology: Current Opinion in Psychiatry April 2008No ratings yetNew Research in Psychooncology: Current Opinion in Psychiatry April 20086 pages
- Prevalence of Depression, Anxiety, and Adjustment Disorder in Oncological, Haematological, and Palliative-Care Settings: A Meta-Analysis of 94 Interview-Based StudiesNo ratings yetPrevalence of Depression, Anxiety, and Adjustment Disorder in Oncological, Haematological, and Palliative-Care Settings: A Meta-Analysis of 94 Interview-Based Studies16 pages
- Mitchell Et All 2011 Prevalence Depression Anxiety Oncoligical HaematologicalNo ratings yetMitchell Et All 2011 Prevalence Depression Anxiety Oncoligical Haematological15 pages
- Psychological Distress in Cancer PatientsNo ratings yetPsychological Distress in Cancer Patients6 pages
- Psychiatric Care for Head and Neck CancerNo ratings yetPsychiatric Care for Head and Neck Cancer15 pages
- The Prevalence, Detection and Intervention For Depression and Anxiety in OncologyNo ratings yetThe Prevalence, Detection and Intervention For Depression and Anxiety in Oncology12 pages
- Anxiety and Depression in Digestive CancerNo ratings yetAnxiety and Depression in Digestive Cancer8 pages
- Psychological Impact of Cancer AssessmentsNo ratings yetPsychological Impact of Cancer Assessments5 pages
- Anxiety and Depression in Patients With Head and Neck Cancer 6-Month Follow-Up StudyNo ratings yetAnxiety and Depression in Patients With Head and Neck Cancer 6-Month Follow-Up Study9 pages
- Emotional Control's Impact on Cancer AnxietyNo ratings yetEmotional Control's Impact on Cancer Anxiety12 pages
- Anxiety and Depression After Cancer DiagnosisNo ratings yetAnxiety and Depression After Cancer Diagnosis26 pages
- Anxiety During Cancer Diagnosis - Examining The Influence of Monitoring Coping Style and Treatment PlanNo ratings yetAnxiety During Cancer Diagnosis - Examining The Influence of Monitoring Coping Style and Treatment Plan19 pages
- Depression Awareness in Terminally Ill PatientsNo ratings yetDepression Awareness in Terminally Ill Patients23 pages
- Predictors of Distress in Cancer PatientsNo ratings yetPredictors of Distress in Cancer Patients11 pages
- Module 3 - Biopsychosocial-Spiritual Effects of CancerNo ratings yetModule 3 - Biopsychosocial-Spiritual Effects of Cancer48 pages
- Psychiatric Morbidity in Cancer PatientsNo ratings yetPsychiatric Morbidity in Cancer Patients8 pages
- Develop Anxiety, Depressioni and HRQOL in Oncology Pts Wo Initial Symptoms HADS - Comparative. SueciaNo ratings yetDevelop Anxiety, Depressioni and HRQOL in Oncology Pts Wo Initial Symptoms HADS - Comparative. Suecia10 pages
- Ja17 A Cognitive Approach To Cancer TreatmentNo ratings yetJa17 A Cognitive Approach To Cancer Treatment6 pages
- Psychological Distress in Cancer PatientsNo ratings yetPsychological Distress in Cancer Patients11 pages
- Psychological Impact of Cancer ExplainedNo ratings yetPsychological Impact of Cancer Explained7 pages
- Anxiety and Depression in Rwandan Cancer PatientsNo ratings yetAnxiety and Depression in Rwandan Cancer Patients8 pages
- Mental Health Care in Oncology. ContemporaryNo ratings yetMental Health Care in Oncology. Contemporary4 pages
- Psychiatric Consideration in Oncology PatientNo ratings yetPsychiatric Consideration in Oncology Patient35 pages
- Depressive Symptoms in Cancer Patients' Final DaysNo ratings yetDepressive Symptoms in Cancer Patients' Final Days10 pages
- Psychiatric Morbidity in Cancer PatientsNo ratings yetPsychiatric Morbidity in Cancer Patients2 pages
- BR J Cancer. Original. HADS Cutoff Scores For Cancer Pts in Acute Care. AlemaniaNo ratings yetBR J Cancer. Original. HADS Cutoff Scores For Cancer Pts in Acute Care. Alemania5 pages
- Psychological Strategies for Cancer CareNo ratings yetPsychological Strategies for Cancer Care23 pages
- Prevalence of Psychiatric Morbidity Among Cancer.7No ratings yetPrevalence of Psychiatric Morbidity Among Cancer.76 pages
- Shim Et Al 2021 Psychiatric Comorbidities and Quality of Life in Breast Cancer Patients Undergoing Radiation TreatmentNo ratings yetShim Et Al 2021 Psychiatric Comorbidities and Quality of Life in Breast Cancer Patients Undergoing Radiation Treatment16 pages
- Anxiety and Depression of Patients With Digestive PDFNo ratings yetAnxiety and Depression of Patients With Digestive PDF9 pages
- Estrategias de Afrontamiento en Pacientes Con CancNo ratings yetEstrategias de Afrontamiento en Pacientes Con Canc9 pages
- MOdelo Propuesto Adaptación Al Tratamiento Del Cáncer Oa La Transición PersonalNo ratings yetMOdelo Propuesto Adaptación Al Tratamiento Del Cáncer Oa La Transición Personal18 pages
- DIsfagia em Pacientes Com Cancer de LínguaNo ratings yetDIsfagia em Pacientes Com Cancer de Língua8 pages
- Afatinib Versus Chemotherapy For Patients With Non Small Cell Lung JCO 2025No ratings yetAfatinib Versus Chemotherapy For Patients With Non Small Cell Lung JCO 202512 pages
- Establishing an Oncology Center in LiberiaNo ratings yetEstablishing an Oncology Center in Liberia9 pages
- Flip Chart 3ok - Breast Cancer PreventionNo ratings yetFlip Chart 3ok - Breast Cancer Prevention27 pages
- Radiotherapy Protocol For Operable Invasive Breast Cancer RT UK V3.4No ratings yetRadiotherapy Protocol For Operable Invasive Breast Cancer RT UK V3.427 pages
- Demaria, S., NG, B., Devitt, M. L., Babb, J. S., Kawashima, N., Liebes, L., Et Al. (2004) .No ratings yetDemaria, S., NG, B., Devitt, M. L., Babb, J. S., Kawashima, N., Liebes, L., Et Al. (2004) .9 pages
- Radiation Therapy in Inflammatory Breast CancerNo ratings yetRadiation Therapy in Inflammatory Breast Cancer22 pages
- Malignancy of Nose and Paranasal SinusesNo ratings yetMalignancy of Nose and Paranasal Sinuses10 pages
- bcc6 Exercises After Breast Cancer SurgeryNo ratings yetbcc6 Exercises After Breast Cancer Surgery13 pages
- 2020 Guidelines for Prostate Cancer TreatmentNo ratings yet2020 Guidelines for Prostate Cancer Treatment20 pages
- Weiss Et Al. - 2013 - Comparison of Prostate Volume Measured by Transrectal Ultrasound and Magnetic Resonance Imaging IsNo ratings yetWeiss Et Al. - 2013 - Comparison of Prostate Volume Measured by Transrectal Ultrasound and Magnetic Resonance Imaging Is5 pages