0% found this document useful (0 votes)
99 views1 pageUCU-CAT Application Form
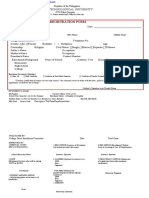
This document is a College Admission Test Application Form for Urdaneta City University for the academic year 2022-2023. It includes sections for personal information, educational background, and required documents, as well as an information consent form regarding the use of personal data. Additionally, it provides details for the examination slip and reminders for applicants regarding the test day requirements.
Uploaded by
thccchcknCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
99 views1 pageUCU-CAT Application Form
This document is a College Admission Test Application Form for Urdaneta City University for the academic year 2022-2023. It includes sections for personal information, educational background, and required documents, as well as an information consent form regarding the use of personal data. Additionally, it provides details for the examination slip and reminders for applicants regarding the test day requirements.
Uploaded by
thccchcknCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd