0% found this document useful (0 votes)
46 views3 pagesDocument 1
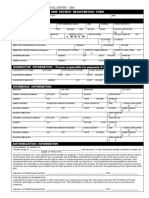
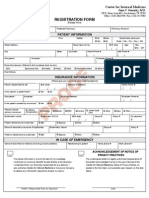
The document is a Patient Intake Form that collects essential information from patients, including personal details, emergency contact, insurance information, referral sources, and reasons for the visit. It also includes a consent section for the accuracy of the information provided and authorization for insurance claims. The form is structured to ensure comprehensive data collection for medical services.
Uploaded by
sooryamkforstudyCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
46 views3 pagesDocument 1
The document is a Patient Intake Form that collects essential information from patients, including personal details, emergency contact, insurance information, referral sources, and reasons for the visit. It also includes a consent section for the accuracy of the information provided and authorization for insurance claims. The form is structured to ensure comprehensive data collection for medical services.
Uploaded by
sooryamkforstudyCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd