0% found this document useful (0 votes)
20 views4 pagesOct 23 With Deng
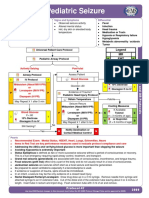
Baby Hospital Miraj provides essential care for neonates and children, including pediatric and neonatal intensive care, cardiology, and neurology services. The document outlines red flags for illness, proper procedures for administering rectal diazepam during seizures, and guidelines for managing dengue cases. It emphasizes the importance of monitoring hematocrit and platelet levels, and lists the hospital's facilities and expert staff available for care.
Uploaded by
childicuCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
20 views4 pagesOct 23 With Deng
Baby Hospital Miraj provides essential care for neonates and children, including pediatric and neonatal intensive care, cardiology, and neurology services. The document outlines red flags for illness, proper procedures for administering rectal diazepam during seizures, and guidelines for managing dengue cases. It emphasizes the importance of monitoring hematocrit and platelet levels, and lists the hospital's facilities and expert staff available for care.
Uploaded by
childicuCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd