0% found this document useful (0 votes)
707 views20 pagesCSF Analysis
Cerebrospinal fluid is produced in the ventricles and circulates through the subarachnoid space. It is reabsorbed in the arachnoid villi. A lumbar puncture can be used diagnostically to check for conditions like meningitis or subarachnoid hemorrhage, and therapeutically to relieve increased intracranial pressure. During the procedure, CSF is collected and analyzed for pressure, appearance, and cell count to check for abnormalities that could indicate different conditions.
Uploaded by
EBCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PPTX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
707 views20 pagesCSF Analysis
Cerebrospinal fluid is produced in the ventricles and circulates through the subarachnoid space. It is reabsorbed in the arachnoid villi. A lumbar puncture can be used diagnostically to check for conditions like meningitis or subarachnoid hemorrhage, and therapeutically to relieve increased intracranial pressure. During the procedure, CSF is collected and analyzed for pressure, appearance, and cell count to check for abnormalities that could indicate different conditions.
Uploaded by
EBCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PPTX, PDF, TXT or read online on Scribd
- CSF Analysis: Introduction to cerebrospinal fluid analysis examining its purpose and procedural overview.
- Physiology: Covers the production and circulation of cerebrospinal fluid within the central nervous system.
- Characteristics: Describes the normal physical and pressure characteristics of CSF, outlining standard clinical measures.
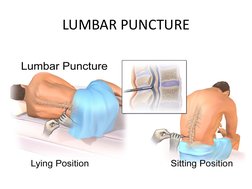
- Lumbar Puncture: Illustrates the lumbar puncture procedure with visuals of body positioning for sample collection.
- Indications: Presents reasons for performing lumbar puncture, differentiating between diagnostic and therapeutic purposes.
- Contraindications: Lists conditions where lumbar puncture is inadvisable due to potential complications.
- Procedure: Describes the step-by-step method of performing a lumbar puncture, including equipment and technique.
- CSF Analysis - Details: Detailed analytical parameters of CSF samples, including pressure, appearance, cellular components, and anomalies.