You might also like
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadNo ratings yet
- Evaluation of A Simple and Rapid Dipstick Assay For The Diagnosis of Typhoid Fever in IndonesiaDocument5 pagesEvaluation of A Simple and Rapid Dipstick Assay For The Diagnosis of Typhoid Fever in IndonesiaFauzi SatriaNo ratings yet
- Clinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapyDocument10 pagesClinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapySuci ZahraniNo ratings yet
- Different Diagnostic Procedure of Typhoid Fever ADocument8 pagesDifferent Diagnostic Procedure of Typhoid Fever AdjebrutNo ratings yet
- Clinical Epidemiology SGD 1Document6 pagesClinical Epidemiology SGD 1Beatrice Del RosarioNo ratings yet
- Diagnosis and Treatment of Typhoid Fever and Associated PrevailingDocument7 pagesDiagnosis and Treatment of Typhoid Fever and Associated Prevailing073090No ratings yet
- Role of Widal Test in The Diagnosis of Typhoid Fever in Context To Other TestDocument3 pagesRole of Widal Test in The Diagnosis of Typhoid Fever in Context To Other TestDrashua AshuaNo ratings yet
- Predictors of Spontaneous Bleeding in DengueDocument4 pagesPredictors of Spontaneous Bleeding in DengueSawettachai JaitaNo ratings yet
- Typhoid JournalDocument7 pagesTyphoid JournalRegina AyediaNo ratings yet
- To Study Haematological Profile of Enteric Fever Patients.: International Journal of Current Research in Medical SciencesDocument6 pagesTo Study Haematological Profile of Enteric Fever Patients.: International Journal of Current Research in Medical SciencesAnonymous hF9HwHVuqNo ratings yet
- Original Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodDocument6 pagesOriginal Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodRidha Surya NugrahaNo ratings yet
- Acute Bacterial Gastroenteritis: A Study of Adult Patients With Positive Stool Cultures Treated in The Emergency DepartmentDocument4 pagesAcute Bacterial Gastroenteritis: A Study of Adult Patients With Positive Stool Cultures Treated in The Emergency DepartmentJuvel PerochoNo ratings yet
- 335 FullDocument4 pages335 FullJinu AuraNo ratings yet
- Abses HeparDocument4 pagesAbses HeparIecHa RizkaMaulidaNo ratings yet
- Carraro 2013 RSBMTV 46 N 2 P 161Document5 pagesCarraro 2013 RSBMTV 46 N 2 P 161Emerson CarraroNo ratings yet
- Differences in Clinical and Laboratory Findings Between Group D and Non-Group D Non-TyphoidalDocument10 pagesDifferences in Clinical and Laboratory Findings Between Group D and Non-Group D Non-TyphoidalBana NanaNo ratings yet
- Infection Status of Hospitalized Diarrheal Patients With Gastrointestinal Protozoa, Bacteria, and Viruses in The Republic of KoreaDocument9 pagesInfection Status of Hospitalized Diarrheal Patients With Gastrointestinal Protozoa, Bacteria, and Viruses in The Republic of KoreaMelia Kusuma WardaniNo ratings yet
- Received: Accepted:: UJMR, Volume 5 Number 1, June, 2020, PP 18 - 23Document7 pagesReceived: Accepted:: UJMR, Volume 5 Number 1, June, 2020, PP 18 - 23UMYU Journal of Microbiology Research (UJMR)No ratings yet
- Thesis On Salmonella TyphiDocument4 pagesThesis On Salmonella Typhikimberlyreyessterlingheights100% (2)
- Jurnal Interna 123456Document9 pagesJurnal Interna 123456vonnyandira28No ratings yet
- Clinical Profile, Etiology, and Management of Hydropneumothorax: An Indian ExperienceDocument5 pagesClinical Profile, Etiology, and Management of Hydropneumothorax: An Indian ExperienceSarah DaniswaraNo ratings yet
- 2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)Document6 pages2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- Attenuation of Sepsis-Related Immunoparalysis by Continuous Veno-Venous Hemofiltration in Experimental Porcine PancreatitisDocument8 pagesAttenuation of Sepsis-Related Immunoparalysis by Continuous Veno-Venous Hemofiltration in Experimental Porcine PancreatitismanuelantoniomenaNo ratings yet
- Jurnal 2Document12 pagesJurnal 2zingioNo ratings yet
- Hospital Management: Bacterial InfectionDocument21 pagesHospital Management: Bacterial Infectionapadanainst7372No ratings yet
- Toxoplasma Gondii Infection and Liver Disease - A Case-Control Study in A Northern Mexican PopulationDocument7 pagesToxoplasma Gondii Infection and Liver Disease - A Case-Control Study in A Northern Mexican Populationhasbi.alginaaNo ratings yet
- Lee, Song, Yu - 2005 - Prevalence of Diarrhea Caused by Cryptosporidium Parvum in non-HIV Patients in Jeollanam-Do, KoreaDocument4 pagesLee, Song, Yu - 2005 - Prevalence of Diarrhea Caused by Cryptosporidium Parvum in non-HIV Patients in Jeollanam-Do, KoreawiwienNo ratings yet
- Eosinopenia in Patients With TDocument9 pagesEosinopenia in Patients With Tnoventina7marbunNo ratings yet
- Health20120100002 44132100Document5 pagesHealth20120100002 44132100Gautam BhallaNo ratings yet
- PPT HiponatremiDocument9 pagesPPT HiponatremiArini NurlelaNo ratings yet
- Jhe2021 6455659Document5 pagesJhe2021 6455659Septi MuninggarNo ratings yet
- Role of Widal Test in The Diagnosis of Typhoid Fever in Context To Other TestDocument3 pagesRole of Widal Test in The Diagnosis of Typhoid Fever in Context To Other TestsimbawulaNo ratings yet
- Diarrhea Associated With Typhoid Fever: ParatyphiDocument6 pagesDiarrhea Associated With Typhoid Fever: ParatyphiNadya Ayu AnanditaNo ratings yet
- AsoDocument10 pagesAsoDiah WahyuniNo ratings yet
- Heparin-Binding Protein: A Diagnostic Biomarker of Urinary Tract Infection in AdultsDocument9 pagesHeparin-Binding Protein: A Diagnostic Biomarker of Urinary Tract Infection in AdultsFitria NurulfathNo ratings yet
- Prevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian CityDocument11 pagesPrevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian CityAna LemesNo ratings yet
- Yield of Blood Cultures in Children Presenting With Febrile Illness in A Tertiary Care HospitalDocument5 pagesYield of Blood Cultures in Children Presenting With Febrile Illness in A Tertiary Care Hospitalfaraz.mirza1No ratings yet
- Research ArticleDocument8 pagesResearch ArticleAliyu labboNo ratings yet
- What Proportion of Salmonella Typhi Cases Are Detected by Blood Culture? A Systematic Literature ReviewDocument8 pagesWhat Proportion of Salmonella Typhi Cases Are Detected by Blood Culture? A Systematic Literature ReviewRansidelenta Vistaprila ElmardaNo ratings yet
- 1382-Article Text-5022-1-10-20180430 PDFDocument4 pages1382-Article Text-5022-1-10-20180430 PDFFadillNo ratings yet
- Blood Surveillance and Detection On Platelet Bacterial Contamination Associated With Septic Events.Document7 pagesBlood Surveillance and Detection On Platelet Bacterial Contamination Associated With Septic Events.Pritha BhuwapaksophonNo ratings yet
- A Double-Blind, Placebo-Controlled Trial of Ruxolitinib For MyelofibrosisDocument9 pagesA Double-Blind, Placebo-Controlled Trial of Ruxolitinib For MyelofibrosisharlessitompulNo ratings yet
- WJH 3 130bacteremiaDocument7 pagesWJH 3 130bacteremiaLasiaf AlaskaNo ratings yet
- Abcesele FicatuluiDocument4 pagesAbcesele FicatuluiMihaela AlinaNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument8 pagesRajiv Gandhi University of Health Sciences Bangalore, Karnatakadsochel999No ratings yet
- Dengue Hemorrhagic Fever: The Sensitivity and Specificity of The World Health Organization Definition For Identification of Severe Cases of Dengue in Thailand, 1994-2005Document10 pagesDengue Hemorrhagic Fever: The Sensitivity and Specificity of The World Health Organization Definition For Identification of Severe Cases of Dengue in Thailand, 1994-2005Dessy AmaranthaNo ratings yet
- Alterations of The Gut Microbiome in Chinese PatieDocument7 pagesAlterations of The Gut Microbiome in Chinese PatieMarcela Garzon O VelezNo ratings yet
- Validity of CSF Tests for Diagnosing Tuberculous MeningitisDocument5 pagesValidity of CSF Tests for Diagnosing Tuberculous MeningitismelisaberlianNo ratings yet
- Blood Culture Booklet - PRN 16 0097a 00 MK Approved13jul161Document36 pagesBlood Culture Booklet - PRN 16 0097a 00 MK Approved13jul161Thiody Hope LimosneroNo ratings yet
- Biology of Blood and Marrow Transplantation: ReviewsDocument19 pagesBiology of Blood and Marrow Transplantation: Reviewsmuhammad fadliNo ratings yet
- Update in TBC and Non TBCDocument5 pagesUpdate in TBC and Non TBCReynaVG19No ratings yet
- Diarrhea EtiologyDocument8 pagesDiarrhea EtiologyEfti WeaslyNo ratings yet
- ManuscriptDocument13 pagesManuscriptMegbaruNo ratings yet
- Fam Art 4Document6 pagesFam Art 4GENETICA CLINICA GENETICANo ratings yet
- Bacterial Etiology of Acute Diarrhea in Children Under Five Years of AgeDocument6 pagesBacterial Etiology of Acute Diarrhea in Children Under Five Years of AgeOmar DoskyNo ratings yet
- Blood Culture Key Investigations BookletDocument36 pagesBlood Culture Key Investigations BooklettahirinicoledNo ratings yet
- PancytopeniaDocument4 pagesPancytopeniaf31asnNo ratings yet
- Salmonella hepatitis analysisDocument3 pagesSalmonella hepatitis analysisWawan BwNo ratings yet
- Escherichia Coli (EDocument16 pagesEscherichia Coli (EDiyantoro NyoNo ratings yet
- Lesson Exemplar: Living Through Pandemics and Public Emergencies Session To Explain COVID-19Document7 pagesLesson Exemplar: Living Through Pandemics and Public Emergencies Session To Explain COVID-19Maria Divina BambeNo ratings yet
- Benito K. Lim Hong III, M.DDocument55 pagesBenito K. Lim Hong III, M.DCoy NuñezNo ratings yet
- Cts-Mdcat 4th Online TestDocument36 pagesCts-Mdcat 4th Online Testjaipal singhNo ratings yet
- Immunization Programme and Preventive Immunization: Presented By: Kanchan MSC 1 YRDocument53 pagesImmunization Programme and Preventive Immunization: Presented By: Kanchan MSC 1 YRArchanaNo ratings yet
- Agility & TestLine SmartKits - AN - 210x210mm - 3Document5 pagesAgility & TestLine SmartKits - AN - 210x210mm - 3Abdalazeez AlsayedNo ratings yet
- Virus or Bacteria - What's The Difference?Document1 pageVirus or Bacteria - What's The Difference?vallabhaneni rajeshNo ratings yet
- Microbial Structures and Functions MoicroorganismsDocument390 pagesMicrobial Structures and Functions MoicroorganismssamsoatsNo ratings yet
- BSC BioinformaticsDocument31 pagesBSC BioinformaticsAjay KumarNo ratings yet
- 1,000,000 AND COUNTING: A July Without Roger FedererDocument16 pages1,000,000 AND COUNTING: A July Without Roger FedererrtNo ratings yet
- Lesson 2 - Classification of DiseasesDocument43 pagesLesson 2 - Classification of DiseasesHanis Joe100% (2)
- Water Borne Disease Signs, Symptoms and PreventionDocument5 pagesWater Borne Disease Signs, Symptoms and PreventionRoxie SilvanoNo ratings yet
- Parasitology Lecture NotesDocument8 pagesParasitology Lecture NotesRica DezaNo ratings yet
- Poxviridae: In: A Concise Review of Veterinary Virology, Carter G.R., Wise D.J. and Flores E.F. (Eds.) - A3410.1005Document10 pagesPoxviridae: In: A Concise Review of Veterinary Virology, Carter G.R., Wise D.J. and Flores E.F. (Eds.) - A3410.1005Mestesanu ElisabetaNo ratings yet
- Chest X-ray Patterns Help Diagnose PneumoniaDocument3 pagesChest X-ray Patterns Help Diagnose PneumoniaVishesh SoodNo ratings yet
- Classification of MicroorganismsDocument13 pagesClassification of MicroorganismsIngrid Amadea100% (2)
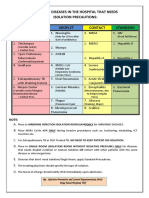
- Common Hospital Diseases Requiring Isolation PrecautionsDocument1 pageCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNo ratings yet
- InfluenzaDocument2 pagesInfluenzajohnndoeeNo ratings yet
- Microbial Associations/Interactio NS: Nanette Ramilo-Cruz, MD, DPAFPDocument50 pagesMicrobial Associations/Interactio NS: Nanette Ramilo-Cruz, MD, DPAFPKhatrinaNo ratings yet
- Causative Agents of Yeast InfectionsDocument2 pagesCausative Agents of Yeast InfectionsDreyden HaloNo ratings yet
- Capitulo 8 EnterobacteriaceaeDocument6 pagesCapitulo 8 EnterobacteriaceaeLuis RodriguezNo ratings yet
- Dengue Bukhar Ka Ilaj Lakshan Karan Bachne Ke Upay in HindiDocument2 pagesDengue Bukhar Ka Ilaj Lakshan Karan Bachne Ke Upay in HindiSumit upayNo ratings yet
- Myco Viro Mod 5Document3 pagesMyco Viro Mod 5Pauline Louise S. DURANNo ratings yet
- Airborne Disinfectant for Room DecontaminationDocument2 pagesAirborne Disinfectant for Room DecontaminationMoussa ElzeinNo ratings yet
- Integ CD TipsDocument2 pagesInteg CD TipsNia KayeNo ratings yet
- HCV PrelimDocument7 pagesHCV PrelimPeter DindahNo ratings yet
- APhA Immunization Module 3Document49 pagesAPhA Immunization Module 3Gerald GamboaNo ratings yet
- Capstone LRDocument7 pagesCapstone LRBrian LuyahanNo ratings yet
- Pamantasan NG Lungsod NG MaynilaDocument4 pagesPamantasan NG Lungsod NG MaynilatipyangNo ratings yet
- Communicable Disease Prevention LessonDocument7 pagesCommunicable Disease Prevention LessonVia Thriss Ann SalasNo ratings yet