You might also like
- 2009al Alami Zestos Pediatriclaryngospasm CurrOpinAnaesthesiolDocument9 pages2009al Alami Zestos Pediatriclaryngospasm CurrOpinAnaesthesiolFernando Feliz ChristianNo ratings yet
- TipsDocument1 pageTipsArchi MakakalikasanNo ratings yet
- CRF BloodDocument10 pagesCRF BloodFernando Feliz ChristianNo ratings yet
- Acute Heart FailureDocument13 pagesAcute Heart FailureFernando Feliz ChristianNo ratings yet
- Algo FibrinolyticDocument2 pagesAlgo FibrinolyticBobo SmithyNo ratings yet
- Acute Heart FailureDocument13 pagesAcute Heart FailureFernando Feliz ChristianNo ratings yet
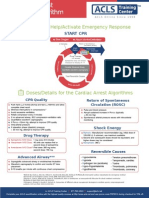
- Shout For Help/Activate Emergency Response: CPR StartDocument2 pagesShout For Help/Activate Emergency Response: CPR StartdavpierNo ratings yet
- 24 CFP Clinical Guideline 10 - Chemical RestraintDocument20 pages24 CFP Clinical Guideline 10 - Chemical RestraintFernando Feliz ChristianNo ratings yet
- Pus TakaDocument2 pagesPus TakaFernando Feliz ChristianNo ratings yet
- Jurnal Physical RestraintDocument8 pagesJurnal Physical RestraintFernando Feliz ChristianNo ratings yet
- Faq (Please Read Before Asking)Document4 pagesFaq (Please Read Before Asking)Fernando Feliz ChristianNo ratings yet
- Kunci Pretes Truncus CerebriDocument1 pageKunci Pretes Truncus CerebriFernando Feliz ChristianNo ratings yet
- Thermoregulation 2Document10 pagesThermoregulation 2Fernando Feliz ChristianNo ratings yet
- Pathogensis - at Risk Populations - Prof Bhisma MurtiDocument21 pagesPathogensis - at Risk Populations - Prof Bhisma MurtiFernando Feliz ChristianNo ratings yet
- Laring EditDocument19 pagesLaring EditSheilla ElfiraNo ratings yet
- Expert Opinion - Ototoxic DrugsDocument17 pagesExpert Opinion - Ototoxic DrugsFernando Feliz ChristianNo ratings yet
- Text LaguDocument1 pageText LaguFernando Feliz ChristianNo ratings yet
- Kumpulan Lagu Guitar Chord ChartDocument6 pagesKumpulan Lagu Guitar Chord Chartfauzi00100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ElderlyDocument19 pagesElderlyrjNo ratings yet
- Leukemia LekDocument17 pagesLeukemia LekErinaGeraldiNo ratings yet
- Part 9 - Apoptosis Cancer and Stem CellsDocument12 pagesPart 9 - Apoptosis Cancer and Stem CellsNL DearestNo ratings yet
- Borderline Personality Disorder Diagnosis Symptoms TreatmentDocument57 pagesBorderline Personality Disorder Diagnosis Symptoms TreatmentAnand KirtiNo ratings yet
- Plowman - 1984 - The Ethnobotany of CocaDocument49 pagesPlowman - 1984 - The Ethnobotany of CocaLuis Flores BlancoNo ratings yet
- Route Route ExtrabolationDocument28 pagesRoute Route ExtrabolationsamfarghNo ratings yet
- AllergyDocument528 pagesAllergyCristina Ene100% (1)
- CAIE Biology A-Level: Topic 19: Genetic TechnologyDocument7 pagesCAIE Biology A-Level: Topic 19: Genetic TechnologysanjidaNo ratings yet
- Epigenetic Theories & StudiesDocument14 pagesEpigenetic Theories & StudiesElizabeth VoightsNo ratings yet
- Mangifera IndicaDocument3 pagesMangifera IndicaRajesh KumarNo ratings yet
- Genetically Modified Foods SlidesDocument18 pagesGenetically Modified Foods SlidesBicycle ThiefNo ratings yet
- Protein Expression HandbookDocument118 pagesProtein Expression HandbookLuis Arístides Torres SánchezNo ratings yet
- Mma DataDocument30 pagesMma DataPau ZalazarNo ratings yet
- NT Biology Answers Chapter 16Document8 pagesNT Biology Answers Chapter 16ASADNo ratings yet
- Arch Forms 1-Ortho / Orthodontic Courses by Indian Dental AcademyDocument48 pagesArch Forms 1-Ortho / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Amelogenesis Imperfecta - Google SearchDocument1 pageAmelogenesis Imperfecta - Google SearchPatitta KulsirirungsunNo ratings yet
- TT2006Document23 pagesTT2006zuz.bienNo ratings yet
- 1 s2.0 S2667031322000355 MainDocument10 pages1 s2.0 S2667031322000355 MainSteffi NotaNo ratings yet
- Intellectual ExceptionalitiesDocument3 pagesIntellectual Exceptionalitiesapi-288159071No ratings yet
- Divan Problems ch16Document3 pagesDivan Problems ch16Merlin MerlinNo ratings yet
- MS ENT Basic Sciences MGR University September 2009 Question Paper With SolutionDocument36 pagesMS ENT Basic Sciences MGR University September 2009 Question Paper With SolutionDr. T. Balasubramanian67% (3)
- Veterinary ToxicologyDocument822 pagesVeterinary Toxicologyying_maggie27100% (5)
- Acute and Chronic DiseasesDocument13 pagesAcute and Chronic DiseasesAchyut AryanNo ratings yet
- The Fundamental of Anti-Aging Medicine: Wimpie PangkahilaDocument44 pagesThe Fundamental of Anti-Aging Medicine: Wimpie PangkahilajujuNo ratings yet
- Technology Debate OutlineDocument7 pagesTechnology Debate OutlineJeremy Keeshin100% (4)
- AcknowledgementDocument42 pagesAcknowledgementKhairul Azmi Mat EsaNo ratings yet
- IOM Pharmacology IDocument93 pagesIOM Pharmacology ISahara MahatNo ratings yet
- Symptoms of Paget S DiseaseDocument49 pagesSymptoms of Paget S DiseaseurufahoNo ratings yet
- Well-Built Clinical QuestionDocument29 pagesWell-Built Clinical QuestionsdghyNo ratings yet
- Antibiotics Actions, Origins, ResistanceDocument344 pagesAntibiotics Actions, Origins, Resistancealery ahreally100% (1)