You might also like
- SOAP Notes: AuthorsDocument6 pagesSOAP Notes: AuthorsRanita Kumalasari100% (4)
- Tendon Transfers For Radial Nerve PalsyDocument62 pagesTendon Transfers For Radial Nerve Palsyavinashrao39No ratings yet
- Shock Study Guide NursingDocument4 pagesShock Study Guide NursingKory Christina100% (2)
- Neurology, Neurosurgery MCQ PointsDocument32 pagesNeurology, Neurosurgery MCQ PointsBruno86% (7)
- Spinal OrthosisDocument16 pagesSpinal OrthosisChristya Ari NugrahaNo ratings yet
- August Neuro CompilationDocument13 pagesAugust Neuro CompilationKoj Lozada100% (2)
- Clinical Medicine Covertemplate: Sports Injuries of The ElbowDocument123 pagesClinical Medicine Covertemplate: Sports Injuries of The ElbowEfrain HernandezNo ratings yet
- Peripheral Nerve InjuriesDocument196 pagesPeripheral Nerve InjuriesAhmad A. Fannoon100% (1)
- Upper Limbs NOTES - BRS Anatomy, Table of Muscles and BRS Questions With Answers ExplainedDocument14 pagesUpper Limbs NOTES - BRS Anatomy, Table of Muscles and BRS Questions With Answers ExplainedJustyna PoznanskaNo ratings yet
- Wrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NDocument46 pagesWrist Drop Claw Hand Median Nerve Palsy: Dr. Srivatsa.NMurali KarthikkNo ratings yet
- Digestive SystemDocument41 pagesDigestive Systemhorace hernandez0% (1)
- Notes Made Easy TraumaDocument74 pagesNotes Made Easy TraumaMorshed Mahbub AbirNo ratings yet
- Asset - 8288 - Anatomy of The Canine Forelimb PDFDocument35 pagesAsset - 8288 - Anatomy of The Canine Forelimb PDFBianca ElenaNo ratings yet
- Brachial Plexus PowerpointDocument37 pagesBrachial Plexus PowerpointMuhammad Naqiuddin JalaluddinNo ratings yet
- Prof DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaDocument77 pagesProf DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaBruno50% (2)
- Dental Office Incident ReportDocument2 pagesDental Office Incident ReportXYZNo ratings yet
- Classification Proposed by Seddon in 1943 Was Generally Accepted But Rarely UsedDocument7 pagesClassification Proposed by Seddon in 1943 Was Generally Accepted But Rarely UsedMd Ahsanuzzaman PinkuNo ratings yet
- Pectoral Region and AxillaDocument25 pagesPectoral Region and AxillaSelva pandi100% (1)
- Portal Lesson 10Document70 pagesPortal Lesson 10Deepak Sugumar100% (3)
- General Surgery 27-03-07Document7 pagesGeneral Surgery 27-03-07Raghu VeerNo ratings yet
- NEET PG 2013 Rank List of Eligible CandidatesDocument256 pagesNEET PG 2013 Rank List of Eligible CandidatesBruno75% (8)
- EU Physiotherapy Guideline For Parkinson's DiseaseDocument29 pagesEU Physiotherapy Guideline For Parkinson's DiseaseAulia Zerlinda SyihabNo ratings yet
- 03 Orlando D. Garcia, JR., Et Al. vs. Ranida Salvador, Et Al.Document2 pages03 Orlando D. Garcia, JR., Et Al. vs. Ranida Salvador, Et Al.Raj AtmanNo ratings yet
- Paid Orthobullet MCQs - AnatomyDocument22 pagesPaid Orthobullet MCQs - AnatomyMohamad Ramadan33% (3)
- Life After Cancer: A Guide For Cancer SurvivorsDocument88 pagesLife After Cancer: A Guide For Cancer SurvivorsjeniferthuyNo ratings yet
- Laryngeal Electromyography Emg Lemg PDFDocument3 pagesLaryngeal Electromyography Emg Lemg PDFSuprit Sn50% (2)
- Lower Limb: Clinicoanatomical ProblemDocument100 pagesLower Limb: Clinicoanatomical ProblemsrisakthiNo ratings yet
- Mahawan Vs People of The Philippines DigestDocument1 pageMahawan Vs People of The Philippines DigestJoy Ann Ferrer100% (1)
- Confused AnatomyDocument3 pagesConfused AnatomyAhmed KassemNo ratings yet
- AnatomyDocument18 pagesAnatomyYoedi YuNo ratings yet
- (OBQ04.162) What Is The Main Blood Supply To The Abductor Digiti Minimi?Document19 pages(OBQ04.162) What Is The Main Blood Supply To The Abductor Digiti Minimi?Yoedi YuNo ratings yet
- Median Nerve Anatomy PDFDocument2 pagesMedian Nerve Anatomy PDFIndra RanteNo ratings yet
- Musculocutaneous Nerve Substituting For The Distal Part of Radial Nerve: A Case Report and Its Embryological BasisDocument3 pagesMusculocutaneous Nerve Substituting For The Distal Part of Radial Nerve: A Case Report and Its Embryological Basis19AYUSHJAINXIISCINo ratings yet
- Week 5 PDFDocument3 pagesWeek 5 PDFnilaahanifahNo ratings yet
- Anatomy Notes 2Document105 pagesAnatomy Notes 2John SmithNo ratings yet
- HandDocument95 pagesHandAsad noor mirzaNo ratings yet
- SAN ZoeDocument5 pagesSAN Zoe2w8qg5qwhdNo ratings yet
- L 9 Anatomy, Nerves of The Lower Limb Lecture NotesDocument15 pagesL 9 Anatomy, Nerves of The Lower Limb Lecture Notesamrwheed9No ratings yet
- LOWER LIMB Understanding ConceptsDocument4 pagesLOWER LIMB Understanding ConceptsAdnan MusaNo ratings yet
- Document 13Document55 pagesDocument 13Kazuya MishimaNo ratings yet
- Safari - Feb 21, 2024 at 12:02 PMDocument1 pageSafari - Feb 21, 2024 at 12:02 PMsyansyncNo ratings yet
- Schumann 1. ExtremiitiesDocument12 pagesSchumann 1. ExtremiitiesCrystal AyalaNo ratings yet
- Human-Anatomy-Kenneth-S-Saladin-2008 (1) - Halaman-424-450 PDFDocument27 pagesHuman-Anatomy-Kenneth-S-Saladin-2008 (1) - Halaman-424-450 PDFBelva EdinaNo ratings yet
- Anatomy - Upper LimbDocument9 pagesAnatomy - Upper LimbjainilNo ratings yet
- Anatomy of The Spinal Cord: A. Cauda Equina B. Conus Medullaris C. Filum Terminale D. Foramen MagnumDocument5 pagesAnatomy of The Spinal Cord: A. Cauda Equina B. Conus Medullaris C. Filum Terminale D. Foramen MagnumChelanie Vidad AndaweNo ratings yet
- 6 Muscles of Forearm FinDocument46 pages6 Muscles of Forearm FinAbdelrhman AbubakrNo ratings yet
- LAB Antero-Medial Thigh & HipDocument10 pagesLAB Antero-Medial Thigh & HipnanaNo ratings yet
- Delorme 1997Document8 pagesDelorme 1997groot marvelNo ratings yet
- LAB Forearm and HandDocument15 pagesLAB Forearm and HandnanaNo ratings yet
- 2 PDFDocument7 pages2 PDFDeei RizalNo ratings yet
- The Brachial PlexusDocument9 pagesThe Brachial PlexusGigi PrexieNo ratings yet
- MSK Assignment NervesDocument6 pagesMSK Assignment NervesMaham TalatNo ratings yet
- Common Pathological Conditions Affecting Movement System Function - HadleyDocument40 pagesCommon Pathological Conditions Affecting Movement System Function - HadleywilliamadiwinataNo ratings yet
- DocumentDocument5 pagesDocumentstella pangestikaNo ratings yet
- Human Anatomy 1Document18 pagesHuman Anatomy 1Phineas MutembeiNo ratings yet
- 805 - Front of ForearmDocument63 pages805 - Front of ForearmUkkNo ratings yet
- A Technique To Identify and Preserve The Spinal Accessory Nerve During Neck DissectionDocument3 pagesA Technique To Identify and Preserve The Spinal Accessory Nerve During Neck DissectionUmer HussainNo ratings yet
- Thopaedic Science: JournalDocument16 pagesThopaedic Science: JournalCiro Madrid FloresNo ratings yet
- ForearmDocument30 pagesForearmAkomolede AbosedeNo ratings yet
- 20-Hip, Knee & Ankle JointsDocument9 pages20-Hip, Knee & Ankle JointsKainat LatifNo ratings yet
- Elective Cases2aDocument156 pagesElective Cases2aMerlin MariandariNo ratings yet
- Clinical Anatomy of The Radial NerveDocument2 pagesClinical Anatomy of The Radial NervemmoslemNo ratings yet
- Arthroscopic Biceps Tenodesis: Operative Technique: Technical NoteDocument3 pagesArthroscopic Biceps Tenodesis: Operative Technique: Technical NoteDaulay AldyNo ratings yet
- A Modified Judet Approach To The ScapulaDocument4 pagesA Modified Judet Approach To The ScapulaGiulio PriftiNo ratings yet
- Tendon TransferDocument6 pagesTendon TransferMd Ahsanuzzaman PinkuNo ratings yet
- Jns 1987 67 3 0463Document4 pagesJns 1987 67 3 0463mohNo ratings yet
- (Journal of Neurosurgery) Retrograde Dissection of The Temporalis Muscle Preventing Muscle Atrophy For Pterional CraniotomyDocument3 pages(Journal of Neurosurgery) Retrograde Dissection of The Temporalis Muscle Preventing Muscle Atrophy For Pterional CraniotomyFaisal AkbarNo ratings yet
- Gross Anatomy of The Forearm: A CAL Package Designed By-Pratik SinhaDocument24 pagesGross Anatomy of The Forearm: A CAL Package Designed By-Pratik Sinhaapi-19916399No ratings yet
- Flexor Tendo Repair and Rehabilitation State of The Art - jbjs2002Document25 pagesFlexor Tendo Repair and Rehabilitation State of The Art - jbjs2002Elfikri AsrilNo ratings yet
- Bachelor Thesis - AmosDocument12 pagesBachelor Thesis - AmosFabianBañoNo ratings yet
- Forearm and Hand - FRCEM SuccessDocument289 pagesForearm and Hand - FRCEM SuccessskNo ratings yet
- Ms Ellaine Boo Role of Trauma NursingDocument35 pagesMs Ellaine Boo Role of Trauma NursingBrunoNo ratings yet
- Physiology and Pathology of Physical and Psychological StressDocument60 pagesPhysiology and Pathology of Physical and Psychological StressBrunoNo ratings yet
- Prof DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesDocument42 pagesProf DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesBrunoNo ratings yet
- DR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonDocument25 pagesDR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonBrunoNo ratings yet
- DR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsDocument32 pagesDR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsBruno100% (1)
- Prof - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenDocument40 pagesProf - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenBrunoNo ratings yet
- DR - Ramana Rao Pre-Hospital Services in Tamil NaduDocument73 pagesDR - Ramana Rao Pre-Hospital Services in Tamil NaduBrunoNo ratings yet
- Mrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNDocument11 pagesMrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNBrunoNo ratings yet
- DR - Joseph Mathew: Trauma Units and Team WorkDocument39 pagesDR - Joseph Mathew: Trauma Units and Team WorkBrunoNo ratings yet
- Hub and Spoke Model For STEMI Management - Tamil Nadu ModelDocument16 pagesHub and Spoke Model For STEMI Management - Tamil Nadu ModelBrunoNo ratings yet
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDocument37 pagesProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoNo ratings yet
- Neurosurgeon For A Social CauseDocument55 pagesNeurosurgeon For A Social CauseBrunoNo ratings yet
- DR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianDocument36 pagesDR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianBruno100% (1)
- TAEI NTRI WorkshopDocument16 pagesTAEI NTRI WorkshopBrunoNo ratings yet
- DR - Darez Ahamed Vision For Tamil NaduDocument6 pagesDR - Darez Ahamed Vision For Tamil NaduBrunoNo ratings yet
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsDocument36 pagesProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoNo ratings yet
- Mr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusDocument25 pagesMr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusBruno100% (1)
- Prof DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareDocument46 pagesProf DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareBrunoNo ratings yet
- DR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemDocument29 pagesDR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemBrunoNo ratings yet
- How Tamil Nadu Eradicated Organ SaleDocument108 pagesHow Tamil Nadu Eradicated Organ SaleBrunoNo ratings yet
- Why Tamil Nadu Model Works Better in Eradicating Organ SaleDocument52 pagesWhy Tamil Nadu Model Works Better in Eradicating Organ SaleBrunoNo ratings yet
- Doctors' Role in Tackling Organ TradeDocument70 pagesDoctors' Role in Tackling Organ TradeBrunoNo ratings yet
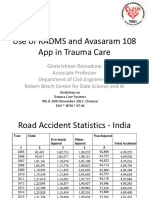
- Prof Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareDocument21 pagesProf Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareBrunoNo ratings yet
- Ian Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduDocument26 pagesIan Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduBrunoNo ratings yet
- TN Gazette 47 of 2013 Part VI Section 4Document84 pagesTN Gazette 47 of 2013 Part VI Section 4BrunoNo ratings yet
- AR Rahman PDFDocument405 pagesAR Rahman PDFPitchai BalaNo ratings yet
- HMIS - Health Management Information System - Government of Tamil NaduDocument12 pagesHMIS - Health Management Information System - Government of Tamil NaduBruno100% (1)
- ATELEKTASISDocument37 pagesATELEKTASISGalih Arief Harimurti WawolumajaNo ratings yet
- InflammationDocument41 pagesInflammationbharath goNo ratings yet
- Clinic Department InfoDocument66 pagesClinic Department InfoHumera ShaikhNo ratings yet
- Brill's Encyclopaedia of The Neo-Latin World: Introduction: Language and RealityDocument17 pagesBrill's Encyclopaedia of The Neo-Latin World: Introduction: Language and RealityIanuarius Valencia ConstantinoNo ratings yet
- WebinabsDocument336 pagesWebinabssacin99999No ratings yet
- AIIMS Question PaperDocument6 pagesAIIMS Question Papersharu4291100% (1)
- Acute Abdomen in Pediatric Patients Admitted To PDFDocument9 pagesAcute Abdomen in Pediatric Patients Admitted To PDFiwanNo ratings yet
- Glycemic Index Vs LoadDocument3 pagesGlycemic Index Vs LoaddominantnatureNo ratings yet
- Intralesional Pentoxifylline Injection in Localized Alopecia Areata 2018Document6 pagesIntralesional Pentoxifylline Injection in Localized Alopecia Areata 2018maat1No ratings yet
- Rs Pena 98 Jl. Pemuda Pengasinan N0.36 Kec Gn. Sindur Bogor Telp: (021) 7587 4401,-FaxDocument61 pagesRs Pena 98 Jl. Pemuda Pengasinan N0.36 Kec Gn. Sindur Bogor Telp: (021) 7587 4401,-Faxrichard fernandoNo ratings yet
- Eng NCPDocument4 pagesEng NCPima nunaNo ratings yet
- ACD/Percepta: Overview of The ModulesDocument91 pagesACD/Percepta: Overview of The ModulesTinto J AlencherryNo ratings yet
- The Anatomical Record - 2021 - Vater - The Topographic and Systematic Anatomy of The Alpaca StomachDocument15 pagesThe Anatomical Record - 2021 - Vater - The Topographic and Systematic Anatomy of The Alpaca StomachMai Chi PhạmNo ratings yet
- 2021 American College of Rheumatology Guideline For The Treatment of Rheumatoid ArthritisDocument30 pages2021 American College of Rheumatology Guideline For The Treatment of Rheumatoid Arthritisjose pablo quero reyesNo ratings yet
- Intracranial NeoplasmaDocument21 pagesIntracranial NeoplasmaLuvi PujiNo ratings yet
- Neurotology Fellowship MilestonesDocument18 pagesNeurotology Fellowship MilestonesAnonymous AuJncFVWvNo ratings yet
- InterRAI Community Health Assessment (CHA)Document10 pagesInterRAI Community Health Assessment (CHA)Mike F MartelliNo ratings yet
- Platinum Gazette 11 JuneDocument16 pagesPlatinum Gazette 11 JuneAnonymous w8NEyXNo ratings yet
- Bacteriological Quality and Safety of Street Vended Foods in Delta State, NigeriaDocument6 pagesBacteriological Quality and Safety of Street Vended Foods in Delta State, NigeriaAlexander DeckerNo ratings yet
- Urinary Incontinence Following Gynaecological SurgeryDocument6 pagesUrinary Incontinence Following Gynaecological SurgeryDwickyNo ratings yet