You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- State of Patriot MissilesDocument13 pagesState of Patriot MissilesTaira Mai100% (1)
- Powerware 5110 UPS User's ManualDocument14 pagesPowerware 5110 UPS User's ManualjulbfuNo ratings yet
- Manufacturing Layout Analysis - Comparing Flexsim With Excel SpreadsheetsDocument2 pagesManufacturing Layout Analysis - Comparing Flexsim With Excel Spreadsheetsmano7428No ratings yet
- VocationalDocument2 pagesVocationalMegha RoyNo ratings yet
- Oracle Exadata Technical Series: Smart ScanDocument59 pagesOracle Exadata Technical Series: Smart ScanVishnusivathej PotukanumaNo ratings yet
- Welding ProceduresDocument11 pagesWelding ProceduresnamasralNo ratings yet
- ME Harmonization Curricilum FinalDocument307 pagesME Harmonization Curricilum Finalratchagaraja33% (3)
- Method Statement of Pipeline WorksDocument13 pagesMethod Statement of Pipeline Worksमनिसभेटुवाल86% (21)
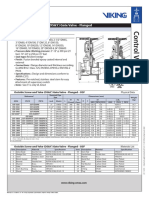
- Outside Screw and Yoke (OS&Y) Gate Valve - Flanged: Technical FeaturesDocument2 pagesOutside Screw and Yoke (OS&Y) Gate Valve - Flanged: Technical FeaturesMark Louie GuintoNo ratings yet
- DP Chipset 15045 DriversDocument592 pagesDP Chipset 15045 DriversRajesh1146No ratings yet
- Technical LetteringDocument12 pagesTechnical LetteringMaverick Timbol50% (2)
- Mix Design Practice For Bituminous MixDocument49 pagesMix Design Practice For Bituminous MixAshwani KesharwaniNo ratings yet
- Powered by QFD OnlineDocument1 pagePowered by QFD OnlineNiswa RochimNo ratings yet
- ASTM C158-02 (2012) Strength of Glass by Flexure (Determination of Modulus of Rupture)Document9 pagesASTM C158-02 (2012) Strength of Glass by Flexure (Determination of Modulus of Rupture)Cristian Perez100% (1)
- Calculation Rail Beam (Hoist Capacity 3 Ton)Document4 pagesCalculation Rail Beam (Hoist Capacity 3 Ton)Edo Faizal2No ratings yet
- 19 Element YagiDocument4 pages19 Element YagiVanessa BileNo ratings yet
- Passive Cooling of The Green Roofs Combined With Night-Time Ventilation and Walls Insulation in Hot and Humid RegionsDocument25 pagesPassive Cooling of The Green Roofs Combined With Night-Time Ventilation and Walls Insulation in Hot and Humid Regionsshailesh gautamNo ratings yet
- Carpentry: Exploratory CourseDocument25 pagesCarpentry: Exploratory CourseJohn Nelson Picones100% (3)
- Sample Electrical LayoutDocument1 pageSample Electrical LayoutBentesais Bente UnoNo ratings yet
- 04 Surveys Cattell PDFDocument16 pages04 Surveys Cattell PDFBrenda MaggNo ratings yet
- Manual Técnico Sony HDC-DX70Document72 pagesManual Técnico Sony HDC-DX70Cristian MoraisNo ratings yet
- Karcher K - 791 - MDocument12 pagesKarcher K - 791 - MJoão Paulo FernandesNo ratings yet
- Acidizing TreatmentsDocument93 pagesAcidizing TreatmentsPeña Lucia100% (2)
- 101.S-4501 Steamer Cyclone Cleaning ProcedureDocument6 pages101.S-4501 Steamer Cyclone Cleaning ProcedureTRONGKIMNo ratings yet
- Mitsubishi 4g13 Engine ManualDocument6 pagesMitsubishi 4g13 Engine ManualJose Luis Caceres Severino100% (1)
- US Hex Bolt SizesDocument2 pagesUS Hex Bolt SizesYana Jarang OlNo ratings yet
- Banda Hoja de DatosDocument1 pageBanda Hoja de DatosSergio Guevara MenaNo ratings yet
- Surface Condenser Eng2Document5 pagesSurface Condenser Eng2MuhammadFikriNo ratings yet
- Computer Organization: - by Rama Krishna Thelagathoti (M.Tech CSE From IIT Madras)Document118 pagesComputer Organization: - by Rama Krishna Thelagathoti (M.Tech CSE From IIT Madras)iamy2ramsNo ratings yet
- Da10 Air Cooled Engine (Appn Code D3.2007 & D3Document26 pagesDa10 Air Cooled Engine (Appn Code D3.2007 & D3Sandeep NikhilNo ratings yet