You might also like
- Genius+ Ba Cu en 1113Document72 pagesGenius+ Ba Cu en 1113AlbertNo ratings yet
- Post Cataract EndophthalmitisDocument55 pagesPost Cataract Endophthalmitisdr samreen arifNo ratings yet
- ARCHITECTURAL ANALYSIS OF POST-TRABECULECTOMY BLEB USING AS-OCTDocument18 pagesARCHITECTURAL ANALYSIS OF POST-TRABECULECTOMY BLEB USING AS-OCTSumit Kumar GuptaNo ratings yet
- Penetrating Keratoplasty StepsDocument57 pagesPenetrating Keratoplasty StepsVishwajeetNo ratings yet
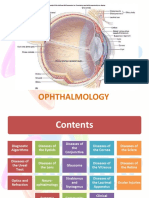
- OphthalmologyDocument144 pagesOphthalmologyrosaririsNo ratings yet
- 5 - Oral UlcerationDocument8 pages5 - Oral UlcerationPrince Ahmed100% (1)
- The M.T Taco Food Truck Business Plan Project Business Plan DraftDocument23 pagesThe M.T Taco Food Truck Business Plan Project Business Plan DraftAbhishek Prasad RoyNo ratings yet
- Ross 308 AP Broiler PO2019-EN PDFDocument16 pagesRoss 308 AP Broiler PO2019-EN PDFJORGE GALVISNo ratings yet
- Diagnosis and Management of Microbial Keratitis: AIOS Guidelines ForDocument24 pagesDiagnosis and Management of Microbial Keratitis: AIOS Guidelines ForKukuh Rizwido PrasetyoNo ratings yet
- Tuberculosis and The EyeDocument16 pagesTuberculosis and The EyeSaid Plazola MercadoNo ratings yet
- 07 - 260CME-Clinical Manifestations of Ocular TuberculosisDocument5 pages07 - 260CME-Clinical Manifestations of Ocular TuberculosisPika LubisNo ratings yet
- By C. Michael Samson, M.D.: Ocular TuberculosisDocument7 pagesBy C. Michael Samson, M.D.: Ocular TuberculosisgigibesiNo ratings yet
- Corneal Vascularization Causes & Management ReviewDocument49 pagesCorneal Vascularization Causes & Management Reviewimran_india12No ratings yet
- Guidelines For The Management of Corneal Ulcer WHODocument36 pagesGuidelines For The Management of Corneal Ulcer WHOichalledhaNo ratings yet
- Catalogue 2019Document201 pagesCatalogue 2019Bima RizkiNo ratings yet
- Tepsorn DissertationDocument370 pagesTepsorn DissertationIsma Angger PambayunNo ratings yet
- Bacterial KeratitisDocument31 pagesBacterial KeratitisMuhammad Rehan SarfrazNo ratings yet
- Syabian skincare glowDocument48 pagesSyabian skincare glowUmiKulsum100% (1)
- Peripheral Ulcerative KeratitisDocument145 pagesPeripheral Ulcerative KeratitisCarlos OrtegaNo ratings yet
- Panophthalmitis: Mbbs KgmuDocument31 pagesPanophthalmitis: Mbbs KgmuDoddy RenaLdoNo ratings yet
- Skill Lab Writing An AbstractDocument6 pagesSkill Lab Writing An AbstractNovi SilalahiNo ratings yet
- Rosacea PDFDocument11 pagesRosacea PDFRio AlexsandroNo ratings yet
- KeratitisDocument70 pagesKeratitisHoopmen Silaen100% (1)
- Juvenile Idiopathic ArthritisDocument19 pagesJuvenile Idiopathic ArthritisMobin Ur Rehman KhanNo ratings yet
- Behcet S DiseaseDocument34 pagesBehcet S DiseaseRendyNo ratings yet
- Stallard's eye surgery pdf free download guideDocument3 pagesStallard's eye surgery pdf free download guideCod Mobile100% (1)
- Assoc. Prof. G. Tomov, PHD: Division of Oral Pathology, Faculty of Dental Medicine Mu - PlovdivDocument106 pagesAssoc. Prof. G. Tomov, PHD: Division of Oral Pathology, Faculty of Dental Medicine Mu - PlovdivAustine OsaweNo ratings yet
- Original Article Factors Related To Filtration-Bleb Morphology After Ex-PRESS SurgeryDocument9 pagesOriginal Article Factors Related To Filtration-Bleb Morphology After Ex-PRESS SurgeryJordi RipollNo ratings yet
- 19 Rationale of Retinal Detachment ManagementDocument87 pages19 Rationale of Retinal Detachment ManagementvajasaNo ratings yet
- Understanding Strabismus PDFDocument143 pagesUnderstanding Strabismus PDFhenok birukNo ratings yet
- Conjunctivitis 161031150615Document282 pagesConjunctivitis 161031150615huzefaNo ratings yet
- Ophthalmology Femtosecond LaserDocument5 pagesOphthalmology Femtosecond LaserChandrika MaluftiNo ratings yet
- Surgical Management of Third Nerve PalsyDocument7 pagesSurgical Management of Third Nerve Palsyhanaddul100% (1)
- Pterigium: Dr. Purnamanita Syawal, SPM, MarsDocument39 pagesPterigium: Dr. Purnamanita Syawal, SPM, Marsyayat muhammadNo ratings yet
- Module Opthalmology Corneal Ulcer: Group 7 Wulan-Fadzely-Arif Amri-Safuan Arif-Nadiah-Insyira-Fatimah-Andi AbsharinaDocument19 pagesModule Opthalmology Corneal Ulcer: Group 7 Wulan-Fadzely-Arif Amri-Safuan Arif-Nadiah-Insyira-Fatimah-Andi Absharinaarifamri92No ratings yet
- Osteomyelitis of JawsDocument28 pagesOsteomyelitis of JawsGujjar VishalNo ratings yet
- Water Drop Splash PowerPoint TemplatesDocument48 pagesWater Drop Splash PowerPoint TemplatesQaulan makrufNo ratings yet
- How to Manage Atopic DermatitisDocument22 pagesHow to Manage Atopic DermatitiszuliaahmadNo ratings yet
- Eyelid Lumps and BumpsDocument43 pagesEyelid Lumps and BumpsAbdul HannanNo ratings yet
- Bullous Keratopathy PRDocument12 pagesBullous Keratopathy PRshevinesaNo ratings yet
- Morphologic Alterations On Posterior Iris-Claw Intraocular Lenses After Traumatic DisenclavationDocument5 pagesMorphologic Alterations On Posterior Iris-Claw Intraocular Lenses After Traumatic DisenclavationYanjinlkham Kh100% (1)
- Atlas Peds Ophthal and Strab Surg SMDocument238 pagesAtlas Peds Ophthal and Strab Surg SMDoina Bobescu100% (1)
- Schirmer TestDocument3 pagesSchirmer TestRisa UtamiNo ratings yet
- Ophthalmology Femtosecond LaserDocument8 pagesOphthalmology Femtosecond LaserChandrika MaluftiNo ratings yet
- How to Form Answerable Clinical QuestionsDocument62 pagesHow to Form Answerable Clinical QuestionsFeniNo ratings yet
- Managing Complications in Glaucoma SurgeryDocument121 pagesManaging Complications in Glaucoma Surgeryshetya_8212No ratings yet
- Morfologi Kelainan KulitDocument67 pagesMorfologi Kelainan KulitLovina Falendini AndriNo ratings yet
- Peran Dokter Umum Utk Kanker Di FasyankesDocument53 pagesPeran Dokter Umum Utk Kanker Di FasyankesChi RahmawatiNo ratings yet
- 10-16-02 Cleft Lip and Palate Part 2 TEKNIKDocument93 pages10-16-02 Cleft Lip and Palate Part 2 TEKNIKSulistyawati WrimunNo ratings yet
- Lens Induced Glaucomas: Saleh Al Obeidan, MDDocument41 pagesLens Induced Glaucomas: Saleh Al Obeidan, MDBhurtyal RajeshNo ratings yet
- Question Bank Is Created As Backup VoluntaryDocument3 pagesQuestion Bank Is Created As Backup VoluntaryD Y Patil Institute of MCA and MBA100% (1)
- Episkleritis Dan SkleritisDocument41 pagesEpiskleritis Dan SkleritisSuryana AdityaNo ratings yet
- Childhood GlaucomaDocument60 pagesChildhood Glaucomaeyemd_in_training100% (1)
- Osteomyelitis: Deo Jake Lacpacan Jhunevyl MallorcaDocument36 pagesOsteomyelitis: Deo Jake Lacpacan Jhunevyl MallorcaDeo Jake Lacpacan100% (1)
- Lens I, Anatomy & PhysiologyDocument67 pagesLens I, Anatomy & PhysiologyNugraha WirawanNo ratings yet
- Gonioscopy 2008 01p001-114 Final PDFDocument114 pagesGonioscopy 2008 01p001-114 Final PDFNsk KhanNo ratings yet
- 14th SOM LAMPUNG 2020 PROPOSALDocument23 pages14th SOM LAMPUNG 2020 PROPOSALnovitaNo ratings yet
- 2006, Vol.24, Issues 2, Women's DermatologyDocument145 pages2006, Vol.24, Issues 2, Women's DermatologyRizweta DestinNo ratings yet
- Ophthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeDocument8 pagesOphthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeAdhe WagiNo ratings yet
- CATARACTDocument25 pagesCATARACTDea NabilaNo ratings yet
- ROSACEADocument19 pagesROSACEAAs Syarif50% (2)
- 80-Article Text-153-1-10-20161118Document4 pages80-Article Text-153-1-10-20161118Rania SalwanabilaNo ratings yet
- Case Report in EnglishDocument9 pagesCase Report in EnglishsashadilanNo ratings yet
- Film Strip Times New Roman FontDocument2 pagesFilm Strip Times New Roman FontBambang AdiNo ratings yet
- Ophthalmology Referral Guidelines: Document IDDocument28 pagesOphthalmology Referral Guidelines: Document IDBambang AdiNo ratings yet
- Clinical and Laboratory Study of Ocular Rosacea in Northern GreeceDocument5 pagesClinical and Laboratory Study of Ocular Rosacea in Northern GreeceBambang AdiNo ratings yet
- Acute Coronaria SyndromeDocument776 pagesAcute Coronaria SyndromeBambang AdiNo ratings yet
- Stye (Hordeolum) Handout (1705 - 0)Document2 pagesStye (Hordeolum) Handout (1705 - 0)Bambang AdiNo ratings yet
- Cheat Plan ZombiDocument23 pagesCheat Plan ZombiBambang AdiNo ratings yet
- 3 3 InterraterDocument16 pages3 3 InterraterBambang AdiNo ratings yet
- Inter RaterDocument3 pagesInter RaterBambang AdiNo ratings yet
- 2nd Semester All Courses-100Document194 pages2nd Semester All Courses-100Ejiade PeterNo ratings yet
- Poisoning: Selenium in LivestockDocument4 pagesPoisoning: Selenium in Livestockdianarbk otuNo ratings yet
- Etabloc Technical DataDocument108 pagesEtabloc Technical Dataedward ksbNo ratings yet
- Chapter 14 The Communist Manifesto As International Relations TheoryDocument12 pagesChapter 14 The Communist Manifesto As International Relations TheoryLaurindo Paulo Ribeiro TchinhamaNo ratings yet
- 43-101 Technical Report Quimsacocha, February 2009Document187 pages43-101 Technical Report Quimsacocha, February 2009Marco Vinicio SotoNo ratings yet
- Psychopathology: Dr. Shafqat Huma MBBS, FCPS (Psychiatry) Fellowship in Addiction Psychiatry (USA)Document48 pagesPsychopathology: Dr. Shafqat Huma MBBS, FCPS (Psychiatry) Fellowship in Addiction Psychiatry (USA)sfrtr100% (1)
- Pharmaceutics | Water Solubility and Dissolution RateDocument11 pagesPharmaceutics | Water Solubility and Dissolution RateAnnisa AgustinaNo ratings yet
- Blower Selection For Wastewater Aeration PDFDocument10 pagesBlower Selection For Wastewater Aeration PDFRobert MontoyaNo ratings yet
- M2030 PA300 Siren Data Sheet 5-2021Document2 pagesM2030 PA300 Siren Data Sheet 5-2021parak014No ratings yet
- Advanced Technologies of CDQ Plant Advanced Technologies of CDQ PlantDocument12 pagesAdvanced Technologies of CDQ Plant Advanced Technologies of CDQ Plant조기현No ratings yet
- ArduinoDocument15 pagesArduinoAlvarez TomasNo ratings yet
- Motherboards Tuf z270 Mark 2Document70 pagesMotherboards Tuf z270 Mark 2Jonah HexNo ratings yet
- CV of Shaila (Me)Document4 pagesCV of Shaila (Me)Masud RanaNo ratings yet
- Toaz - Info Chemtech Reviewer PRDocument1 pageToaz - Info Chemtech Reviewer PRchristy janioNo ratings yet
- Canadian Wood Council Publications and Tools For Wood Design Robertson RocchiDocument62 pagesCanadian Wood Council Publications and Tools For Wood Design Robertson RocchiDj MacNo ratings yet
- Service and Repair Instructions: Water & WastewaterDocument72 pagesService and Repair Instructions: Water & WastewaterLa Marina Mantenimiento100% (1)
- Grade 9 Unit 1 - Part 1: Square RootsDocument20 pagesGrade 9 Unit 1 - Part 1: Square RootsWilson ZhangNo ratings yet
- TED BENTON: Is Capitalism Sustainable?Document2 pagesTED BENTON: Is Capitalism Sustainable?api-25932856No ratings yet
- Analytical Chemistry Lecture Exercise 2 Mole-Mole Mass-Mass: Sorsogon State CollegeDocument2 pagesAnalytical Chemistry Lecture Exercise 2 Mole-Mole Mass-Mass: Sorsogon State CollegeJhon dave SurbanoNo ratings yet
- Briefing Paper No 4 CV Electrification 30 11 17 PDFDocument5 pagesBriefing Paper No 4 CV Electrification 30 11 17 PDFAlex WoodrowNo ratings yet
- Dasar Eksitasi Pada GeneratorDocument8 pagesDasar Eksitasi Pada GeneratorTeknisi Abal AbalNo ratings yet
- Your Song RitaDocument1 pageYour Song Ritacalysta felix wNo ratings yet
- Scheme of Valuation and Key for Transportation Engineering ExamDocument3 pagesScheme of Valuation and Key for Transportation Engineering ExamSivakumarNo ratings yet
- Marketing Strategy of Air-Conditioning Companies: Project SynopsisDocument13 pagesMarketing Strategy of Air-Conditioning Companies: Project SynopsisSrikanta ChoudhuryNo ratings yet
- Experimental Design and Optimization MethodsDocument38 pagesExperimental Design and Optimization MethodssudalaiyandiNo ratings yet
- WPS Ernicu 7 R1 3 6 PDFDocument4 pagesWPS Ernicu 7 R1 3 6 PDFandresNo ratings yet
- Making Soap From WoodDocument6 pagesMaking Soap From WoodmastabloidNo ratings yet