Chapter .3. Thermal. 'effects 'Of incendiary weapons on the human.
body
I. lntrod'uctio.I'l'
A vital ceasideration i.n argiUments about miHtary necessity versus humanitarian prioriries is the medical aspect of the use of incendia_ry' weapons .. Such q,uestiDns as the nature .of the casualty ,eiIeds, the prDblems, of medical treatment, •. he prospects for tlileurviving casuahies, and l.he likelihood and the time of death are all relevant to any asse sment of the 8ft10UrU o.f suffering cau ed tnvictim of incendiary attack .. From the viewpoint. of th.e intemaeional laws of war, this amount ,of _ uffering has somehow to be weighed against the "military necessity" of the use of incendi,· ary weapons, for it is presumaely only in this way that it may be determiaed whether allera part oethis suffering i , "unnecessary" ..
The traumatic effect ,.of mot weapon is topeneeate the sldn and! damage internal organs. Although the acsion .of flame weapoa . is essentially to damage only the skin, fire may cause death ina number of w.ays so that the exact cause may be difficullt to determine in a given case. In gcnera] , death by fir·e may be due to' thefoUowingcau e: (a) hearseoke, caused by the transfer .of heat to the body suffici.ent to increase the body temperature above a critical level (apprQ)::imal~ely 4lOC), (b)pulmDnary damage due to inhalation of make aad toxic fumes. (c) carbon monoxj~t.e poisoning, (d) depriva.ti.on .of 0. ygen, and (e) seventy of the bum wound in terms ofdep,th and the extent of the body sutface area affeceed,
The likielibood of death from bum wounds i aI!so affected by . uch factors as the age, the general heahh and the nutritional. status o.f the victim. and. the potelil.tial risk ·ofinfection. . ._,
Heaestroke may bean important cau e of immediate death from fire, bUI it j . noE, a,ignmcant cause oflater death. The same applies to earbon monoxide poisoning and thedeprivaticn of oxygen, since these reactions are abo reversible (a:I[hough some 10llg~itenn il\iury may result: see Chapter 4). Major factors related to the death rate from bums. after initial
urvival, are the degree of pul1monary injury and the extent of the body surface area involved. The age of tile patient and his general health. and n.utritional status are additional factor which may wnfluence the progneSI . One analy is of the complications causing Oil' contribuHng to death due to buras is shown in 'table 3. L
. Where [oxic and respiratory complication are not present, the mortality from bum in mdlvidualsof giv,en age and general health depends pri-
122
I 18
19
:Baeunall cnmpUcatWn ' Septicaemia 'Bronch.opneumonia, Pyelonephrili Meninpjiti.s
Peri toni lis
:Entero.col illS
0.3'5 gang!iem~ Ex.lra-renal abscess,
t:oUl bacterilal compUcaUoru,
Num,berojcaSi!$
Tlllble 3.1. Complications rrom bUI'n1.ng wbl.ch eaused or eontributed 1.0 deaib
Number ,a/coses
Non,bKte:ril1 £.ompU(.a.tions, Earl.yhock nnd/orcardiac failure Earlyllyperkalaemla
, ther hock
Subtotid
Res piratoFlI c.omp:1i.calions
arben 'IllOI1.oxide Inhal'ation of smoke Glouicbums
Obstructive tracheobronchilis Blast injury to lung Congestive ateleeta i Nlmonary,oedema Inhalation of vomit
ubtotal
A.cute cardiac complic3.lion T,oxic myocanlilis Cardiac arrest
Subtotal
Renal failure Hypokalaem!EI PUtmana.!'), ,emboli III
Hepatlc jaundice . Acute dila.ta~ion ofllH~ tomato
Paralytic ileu , . .
Agranulocytosis lind thrombocytopemB Haemorrhage from acute du denal ulcer Anoxic eerebral -oftening
Subtotal
1 .3 4 2 I III 2 2
lS
4
5
24 '* 5
2 3 I I I I
42
Total oon·bacterUII eompUc.adOIt!!,
T,omlall £ase5
Source: Sevin (1966).
marily UpOD. the depth and extent of the bum. because of the physiological importance of the skin as a. vi~,al ,.organ of the bod.y. This is true whether death results from iinadequat'ely treated shock in the early t.ages of burn care, ubsequem infections or other less frequent causes of dea1th such III bum-induoed gastric ulceration. Except for etectricld bums"ch~~cteriZl~d by the deep destruction of oru des and other l~S ue. but .~th tim1ted. '. kin damage the causative a.gent is lea "important In de1ier:nurungtheoudook
for a bum patient. .. . . . ." . •.. .. . .
For the e reasons. the m~jor thermal effects ·of mcendlary weapons ~n
the human body to be described in this c.bap1ier relate to bum of the S~1D, althougb reference is also made to the so-called "p~mona:ry burns" : whIch have now been shown to be due more (,.0 theillhalauon of smoke, ~nd fU,~e than to actual thermal bum of the lungs. The. ~oxic effects ofmcendlluy
123
weapons are described in chapter 4 where further reference i made to lung irritant effects.
It i somethnes useful to distingui h between pr.irna,ry bums, due to the direct effect of an incendiary agent on the body I and econdary bum , due to the ombu tion of clothe • equipment. house, and oon.Primary bum .. caused by miliitaryincendiary agentsare :Iikelyto be e peciaUy severe since they are the r ult of extensive technol gicaJ efforts to increa e both the heat of combu tion and the burning time. Secondary burn resulting from incendiarie are in principle little different. from bum experienced in civilian lite, about which there is a voluminous medical literature. En thi chapter, the general medical literature on bum j urveyed in order t . convey orne indication of the complexity and severity cf the bum wound and the resulting demands n treatment. facilitie e » Morepecific effects of the use of incendiary weapon are al 0 described. The chapter conclude with a di cu i n of orne additional factor which complicate medical treatment-and therefore the prognc L for the patient-in wartime condition.
II. Pathological effects of bums The kin a a vital organ
The ignificaace of the phy iological role of the kin i not. commonly appreciated. The kin i not onlyan e ential part of the body, but it al 0 ha can iderable p ychological significance to the individual. In both case thi is because the kin forms the ineerfaee between the individual and the outside physical and social world.
A living organi m may be de cribed as an 'open y tern" maintaining it elf in a. dynamic equilibrium with it'. environment Th:i .e.quiUbrium .. , known a homeo ta i ,I i maintained by balancing man.y pre e. ineluding the inge tion of food tuff and the excretion of waste products the inhalation of oxygen and theexhalarion of earbon dioxide, and the imbibing of water in order to com pen ate for the 10 f moi ture by evaporation or excretion.
The skin playa. vital role in maintaining borneo ta i particularly in controlling the temperature of the b dy and inlim:iting evaporati 0 f moi ture from it. When fo d i metabolized in the body it pr du e heat enabling the body to maintain the normal temperature f about 37°C. The kin . cts as an in ulating layer. actively controlling the 10 of heat [0 the urrounding air, and thereby diminishing the f od intake needed
imply to provide the body' "central heating".
I H m('O$1(I.I";.I': he maintenance of 8 . LIe of equilibrium within the body with re 'peel 10 temperature. heart rate, blood pre ure, water content. blood ugar level, and 0 on.
124
Preventing water from evaporating from the body i important for three main rea ons, ir t, evaporation ha a cooling effect. Without control by tile kin the heat Io . due to evap ration placesexce ive demand on the body capacity to generate heat by rnetaboli rn. Second, water j
e sential f r the tran port f ub ranees in the body. If water i lost by evaporation, the body fluid become more concentrated, and in an eff rt to res tore the balance, water pase out of the cell into the fluid urrounding them, and may be lo-t from the b dy by further evaporation. The cells can only tolerate a minor water 1.0 before they die. Third. the effectof the 10 of water whether due to the 10 of circulating blood from damaged blood ve el or by evaporation from open wound I i to decreae the flow of fluid through major organs uch as the brain, heart and kidneys, threatening thee major body systems with injury or death.
Further. the skin i a major means of contact with the environment, containi.ng nerve ending which provide the brain with a continual feedback of in~ormation about pain., temperature, ~oucb and pressure through proprioceptive en ors. If the skin i removed. the e en or are removed with it depriving the brain of much of the information nece ary for adaptive behaviour.
Although much f the kin i u ually clothed for ocial and practical
reason, it has great p ychologica1 importan for the individual ince
being the outside of the body. the. kin i mo t <Ieee ible to ob ervalion and touch by other per on . Damage and deferrnityto the kin, partieularly in uch important areas a the head and hand have far-reaching psychological. can sequences.
The kin i made up of everal layer'. The outer layer, the eplderfl1i , i compo ed of non-living, hard-wearing cell and inome parts of the body, uch a the ole f the feet, may be quite thick. As these outer cells are worn away, they are con ta:Rtly replaced by cell from the underlying layer, called the dermis. Thi layer i compo ed of living cell ~nd contain all the functional components of the kin- mall blood capillaries, nerveendings, sweat giland . and hair full ide .. Dilation, of these blood capillarie enable the body to increase the flow of blood at the surface of the body, where heat L more readily di ipated, Contraction of these ves-
tels helps to con erve the heat of the body. Changes in the tate of the e blood ve sel are re ponsible for changes in the colour of the kin when. a per on i too hot or too cold. Per piration from the weat gland is another mean. of di ipating heat from the body, while the hair i a. means of con-
erving heat. albeit one which islargely ve tigial in man.
Underneath the skin i a layer of adipose ti sue, made up largely of cells containing Large globule oHa.t. which also protect and in ulate the body .. The thicknes f thi layer varie con iderably from one individual to another and in different parts of the body.
St n & Green (1959) howed that the receptor in the kin which are
125
effective in mediating the pain sensatien have III thre hold of approxi~ ma.lely 43~:C.
In a. major series of experiment Moritz and hi colleagues {Henriques & Morilz.1947;. Moritz ,& Henrique 1947; Moritz" 1947)-how.ed thatthe lower temperature limit for a cutaneous bum due to hot water i .approxjma'ely44°C.
At 44"Cit !iook about three hOUfS to raise [he temperature of the undedyin8 skin at. the dermis-fat interface to 44"C. damaging the full thickne s orthe skin. Ala temperature of 55"C, it took only 0..4 :minutes to createthe Same ·effect At lOO"C it wok only some O.leconds to de troy the epidermis, bur in that short time there was 110 significant temperature increase at the dermis-fat interface, That is. thephy iologica:i changes ln the kin due to bums depended UPOO! both the tempemtuflea:nd the time of contact with the buming agent; tbe hotter the agent, the' horter the contact thue re,quired to deslroy the tissue.
It wilill beobvious from the deseription of the functions of the _kin that the severity of a cutaneous bum wound depends not only upon the depth of the bum but al 0 upon tile extent of the body mrface are.a.af~ fected, which determines the 1.0 .of fluid and heatand therefore the irnpact on the majorphyiologicaJ·. ystem of the body.
The depth of burns (degree)
Bums which onl!y il\iure the epidermis, such as mild unburn, are known as first degree burns (see figure 1.1:). They :resulit in temporaryerythema (re;dnes· ), due to dil:alion of tll.e capillaries, and oedema ( wening).They usually heal within a few days after sloughing off the epidermis, and leave no scar.
Buras which extend into the living lay,er ,of the skin. the dermis. are much more serious .. It is common to distinguish between second degree. or_partial thicknes , bum, and 1I/1'rd degree, or full thickness. burns, Second degree bums denote those in which necrosi 2 extend into the dermis, but with the urvival Df a su:ffici:ent €oundati.on of such skin appendagesas sweat glands and hairfioUicies toensure that the skin regenerales without having to heal from the edges of the, wounds. There is a wide var.iati:onlll.tbe severity of these bums. Some. such as severe sunburn with blistering., wtU heal within a week or two and leave no scars; others will heal within a. month with reasonable care: and stilil. others will no~ heal sponcaneously unless specific treatment is ginn to prevent the destruction of survivi.ng ,epithelial" cell of the skin by secondary infection and to encourage these cells to grow. Third degree or filii. thiekne .bums are those ilD which a1Jtbe dermis is, destroyed.
I Necrosis: ['he death of one or more cell Of a. :ponioll of a tissue or organ.
3 .E;pilludirm!: A thin layer of tlis ue without blood ve sel which coversaUi the free surfaces of the bod.y, including eyes, glands, respiratory passages, and so on.
1:26
Figur,e' 3.1 Scbemat:ic outline of (;-Itoss-sedtonof tbe Idn sbowing d:egrees of bum"
'Fi~61: de:gree bum
Second degree' bum
Third degr,e9 burn
.... ifiIiIIi.._- Sulbcutllneou ' f·!!t tissue
follldle ,glandl
capillaries
endIng
• irst degree, ofuperficia'i buras, invo'iveonly the epidermisand heal I~apidly. Second degree bum darnagetbe upper part of the' dermis but i lei, ef living dermattissue remain and proliferate to cover 'the area it! :aboUll4 days. Third degree, d'eep .• er fIJU!hick:lles ,bums e tend through the d rmis and may extend to underlying [i ues, Some authors refer 10' bum which extend into underlying tis ue a fourth andfifih degree bum . In general, UJird degree burns greater {han 1-2 cml in area I"!!Q,uirekintran plantation in ordu to, heal.
In addition there may be destruction of the underlying fat. muscle. bone and other tissues. The terms fourth and fifth, degree burns are sometimes used to describe sucll inj,uri.es.,althollgn in general this nomenclature is no longer favoured in the int·erna:tiona:l litera.tllJre, as speclfi.c deeper injlllri.es of'this sod are beUer recorded a uch.
The depth of the bum is easily misjudged and depends upon the cause, the temperature, the length of e.xpo urevand tbethickness, .of the sk~n (the, soles of the feet, the paIDm - of the hands, a:nd the back being thicker than elsewhere). Intense heat over 3 .• short period may produce a bum which looks very much dike one produced by less beat over a longer period, although the IlaU.er may de troy more of the underlying dermal elements, Both first and _uperfJdaI second degree bums blanche on pres-
Uire with an ins~nllrteJiltueh as a sterne m:i.croscope . lide; the colour returns when t:he pressure is released. Third degree bums do not blanche orflush 0111 pressure or release. The persistence ,of sensation, which is easily tested with a. st,erite needle, is often helpful in differentiating . econd and thiird degree bum , although th.i test is not completely reliable, Destructjon of the fuU skinthickness kiUthe nerve endings,resulting in loss offeeling (Pbillip- & Con table, undated], Bvenexperts 1IDli)' have difficlLdty
W27
in estimating bum depth. and ubequent epsis" may invalidate initially correct judgemen by converting a econd degree bum to a full thicknes i.nJury. Thi is pa:nicl!.liIaily likely to happen ill1, malrteuri hed anaemic patients. who al 0 commonty have no ace to adequate medical facilitie . Deep econd degree bum- often heal with evere earring.
Deep bum, heal only after the dead tis ue i removed eilther by unas i ted or natural eparation, which usually inv lve bacterial infectien, or by repeated dre ing (debridement) or surgical exci ion. The 'clean' bum: wound may then heal by epithelial ingrowth from the edge, if it i Ie s than m-2cmz in area, by theeffecti.ve urgical closure of small wounds, or by the application of kin graft from other parts of the b dy.
The cropping of kin gr.aft leave painful donor ites, comparable to econd degree bums, which u uaUy heal in about two week with no more
than minimal scarring. nder Ie tban optimal c ndition , however.
ep i may intervene and the e donor ites, in turn, become area of full thickaes or third degree skin 10 '. Thi may account for the reluctance of surgeon to apply kin gr (1 to bums which otherwi e appear to necesitate them when patient are in poor condition and medical facilities are minimal. At present, permanent skin graft can only be taken (mm the recipient him elf, identical twin excepted.
econd degree burn are characteri itically extremely painful until they are esentially healed. Third degree burns, becau e of the de tructi:on of the nerve ending in (he dermi are characteristically not trikingly painful: during the fIT t few day after the injury. With progre ive healing and removal of the in en itive overlayer of dead ti ue, the wound become m re and more en iuve until covered with graft or by the: ingrowth of epithelium. Daily changes of dre ing are e cruciatingly painful. equivalent to tearing off the outer, insen Hive layer of the skin from the inner
. en itive layer.
Tbe extent of burns
The second factor determining t:he everity of bum i the extent of the b dy surface area involved, which i igniflcant for everal rea on. The greater the area f kin de troyed, the greater the Jo of moi ture and heat by evaporation, whichare major factor in the pathophysiology of the bum. injury. Second, the greater the area involved, the greater the problem of coping with infection. Third, the greater the area of skin de troyed, the les kini available for grafting-a procedure which i_ all the more nece sary, As a re ult of the e and other fact there i . a direct relation-
hip between the extent of a bum f a given depth and the chane f ur-
• Sepsis: The localized or uperficial presence of variou pu ·forming lind other pathogenic organisms Of their to ins which kill the Ii ues, The presence f mi ro rgani ms or their to in in Lhe ireulating blood may give ri e [0 y temic discs e, a condition known II septicaemia.
128
Figure 3.2 The rille of nin .. as a method ror estimating the approximate extent. of bums In an adult
9%
9%
ource: After Berko (1924).
vival. A convenient mean of estimating the extent of body area burned was introduced by Barkow in 19'24 and i often presenteda . the "rule of nine" (figure 3.2. The face, r an arm make up approximately 9 per cent of the total body urface area whereas a. leg, the front (che tand abdomen together) or the back each make up about 18 per cent. a multiple of 9. The prop rtion are only approximate and are omewhat different for a child. under five years of age (see table 3.2 . The palm of the hand and finger make upab ut W pCI" cent of the bedy serfacearea, 0 that the extent of the burn may b measured approximately by the number of "hands" required to cover it.
Tbe severity and mortality of burns
A· a rough guide, third degree burns of Ie than 5 per cent of the body surface area may be regarded as, tight. wbHe those of more than. 1.0 per cent or first and second degree bums of more than 30 per cent, are regarded as severe. In addition. any truro degree burns affecting the face, band ,5 feet andgenitelia we clas ified as evere, a well as circumferential
Ii Bum of tb.e hand account for .apprQximalely one-third and bum of the face for approximately one-quarter of all burn (Tubiane, SalIX & Kenesi, 1967; Coover e, '1967; Kovanc. Aaby. Hamil & Hardway, 1969). See table 3.10.
129
9-743168
Table 3.2. Methods of ca]nJating approximate extent of bums over bod ·~ul'face Percent
Surface area formulae
rea. of body
surface .
Adult or ch i Id over 5 yrs.oi age
Rule of nine
hild under 5 yr Drage
Head
nterior trunk
P tenor trunk Bolh upper arms Both forearm Both hands
Bolh [highs.
inc! buttocks Both leg
BOlh feel
6
18
20
7.S 1
6.0 18
4.5
/9
Il.O} /9
6.0 15 / 20
9 II ]=18 1/ .2=/8
1/ eac.h=18
II each=?
1/ each=l8
vi/Tee: Phillips lind unstable [undntcd).
deep burn of the limb which affect the circulation to the e trermtie Arturson (1966} add to the cat,egory of evere burn those whieh are complicated in the following way: (a) oft ti ue wound and keletal damage; (b) complication of the respiratory pas a ge; (c) electrical bum ;. (d), imulta.neou radiation injury, and (e) burn wound due to white phosphorus, mu tard gas, or other chelni.cal .
First degree burn have no ignificant mortality. Superficial second d - gree bum. , however extensive, are rarely fa tall if orne medical careuch a that sufficient to maintain an adequate fluid intake in a hot climate, i . available, Thepercent .. age of deep second degree and third degree burn in a given individual can be combined for practical purpo e in e timating probabl:e mortallity, although the mortality from the third degree bum will generally be greater. With adequate treatment, deep econd and third degree bum. of les than IS per cent are unlikely to cau e death. whereas bum of over 50 per cent often do cf. Bull & Squire, (949). With ideal treatment young adult with burn of up to 85 per cent of the body including 70 per cent full thickne burn, havesurvived (Birke, Uljedah1 & Nylen. 1970).
tn general, there is a tati tical relationship between the extent of the bum and the mortality. which i sh wn in figure 3.3. The igmoid relati nship has been not d by a number of author .uch a Clark on & Lawrie (1946). It implie that even for relatively mild bum (e.g, 5-15 percent in adult. aged 15-44 year ) a few individual . Ie s able to withstand the phy iol gical tre e r ulting from burning will die. A imilar rei ti n-
hip bas been noted in the case of some other biological phenomena, uch a the relation hip between mortality and the do e of t xi drug (cf. Gaddum, 1933). Acceptance of the idea of a igmoid relation hip be-
no
Figure 3.3. ChaTacler.i tic relationship betw en mortality and e ertt of burol!l Mortality
tpercenn 100
100
80
60.
(1<11--- Chatacte~istic mortality curve
40
20
o '_
80
20
60
Area burned (per cent)
" The figure iUu trate the typical relati n hip b tween the per entuge of patient !lying {Ihc rn _ rtality) and the II erage area r the bod urface burned. \. hich is II. me sure of the severity of the bum. The. data are averages drawn from vari us groups fpllflients' etween 1:5 and 44 year old (tolal ample=l II patient ).
b The real dam appro lmate 10 an ideal UNe. indicated by Ihe pr, bit fit. II i .1 Slimed that the larger the number of data, lind con equently the larger the number of point it is po ible to plot. the more the actual data would appr rich the ideal igmoid distribution.
lource: Bull & quire 11(49).
tween mortality and bum everit i of great clinical importance, ince it ugge 1 that. in theory some pr bability of urvi at r main even for the rnos t eriou Iy burned patient,
Thi .. ,. i 'preferable to the old idea that II burn of a certain proportion of the body urface wa nece arily fatal. .If each burned patient i regarded ha ing a chance of recovery. every effort will be made to help by mean of treatment (Bull & Squire, 1949. p. 171).
A mathematical method of analy i . known a probit analysi . wa et out by Bli (19 8). among thers, and developed by Finney 1947. The method was fir t applied to burn data. by Bull & Squire (1949) and i nOW common practice.f It enable e timate to be made of the everity f a burn likely to produce any level of m rtality. For in tance in Bun & Squire' original data figure 3.4) a 51 per cent: bum in the 0-14 age gr up was likely to
8 Bull & Squire (1949) de cribed the rati. nale forthi rneth d and con tructed an actuarial table from their data for the pr bahility of death (the m rtallty Ii k) fran. individual f given age and area of burn. BuU & Fi her (1954) publi hed revi ed estimate for calculatin the m rtalityri k which have ince been u ed as a standard of compar.i, on wilh other tudie .
1J,1
Table 3.3. LA~", fO.11 some' .llIrge Ireaimeni sertes
Birk.e & Uijed'ah'l (1968) plasma iJf,fJ/qJB. J96(J...6()
Mg,ure 3.,4., Typieal :mor-CaUty ,ClInes ~death-: In per ,cent) for burned patlent!l ,Ba:ord!· ling to age and extent of buro'l
A~ea bu:med'(par cent].
100 _
!!'ruin
el' al.
Bull Bull ,(11964)
BalC.ter & (11971) (1971) be/ore
hire Bull & be/ore after utpha-
Age (1968) isher AI.' 0'3. AgNO., m ION,
[year l .~(JUf!'.!! !l954j 1944-64 /965-70 19S(J...60
under 15 36 49 4 64 49
I ..44 27 46 47 :56 56
45-64 :lJ 27 29' 40 29
over 65 7 1,0 10 117 Birke & Liljedahl (1968) dextra« group A, 1954-.59
75 ,64 54 30
45 43 6 :13
Stmrc«: Birke &. Liljedahl (19711.
produce de-ath in 50 per cent of the patient treated. The great advaatage of this method i ' that it enables an asses ment of the effectivene .of treatment to be made by comparing the actual mo.r,tality with the pr.eciicleci ,mortaliry from the probitanalys! c. Further e . Bull &. Squire suggested that
justas the tOldcity ora drug is best expreed,in term of the doe needed 10' kill 50 per cent of a. batch of experimental animals (U lIallyknown asthe Lethal Do e of -0 per cent or L. D. 50). 01 we may assess tile treatmentof <J series o:r burned p.alient ill terms of the area of bum prnducing death in .:'JOper cent of ca es (i.e. Leilia! Area for 50 per cent, or LA. 50), (Bull! & Squire', 1949 •. pp, 166--167).
_ hal: is, the greater the LAM)' the more . ucce sful the mean of treatment, Table 3.3 show the lie ults of a eries of studies by different author, orne of which indicate progress in the treatment of burn: a new methcd were :inlroduced.
The inflnenc,eof age ODI .morlaUty
The age ·of the patient is a major faetorin the rnortaiity of bum, with the elderly surviving bum le s effectivdy ( ee figure 3.5). A very rough rule for adultpatlen! i that. :if the age of the patient and the percentage of the body urfa.c·e area burned added together exceed 100 then urvival i Unlikely .. For example, a 50~year~old patient with a 40. per cem bum may hope to urvivetan 80~year·old patient with a 25 per cent bum. ii unlike~y to do so ..
• mn the mortality data provided by Bull & Squire U9'49')., all children within the age group ()...·14 were classified together, and these data indio cated a relatively good capacity to survive buminjurie . ,( ee figure 3.4)" Other author, by contra I, believe that very young children lIave less a.bility to urvive bums than do, young adult. Dataprovfded by Pruitt. Tumbe ch, Mason & Pearson 0964) confirm uch a view,and these author ugge ta posibleexp]ana.tion,
The present data 011 (Ile young~r age groups (0-4 and ~14) ... would sugge t thaI these younger groups are able 10 with tand bum illjU"1F}' of upto 30 per cent ofthe 'body surface virtually as well a the older groups. Beyond that level. how-
1.:12
O.._-..J ............. ......".,,....-....,J,--~--:=--.=-~
, 0 20' 3'040' 50 60 70
A'ge' (vears)
• Data from 1100 patients treatedat the ~ S Army· urgieal Research Unit. 19 0-1960.
$nllfce: Pruitt, Tumbusch, Ma .. son &P:ear on ,[ 19M}.
ever, thisgroup appear :ignificantly ~I'e-sabl.e to withstand comparable percentage, area bums. The large area to weight ratio in children may expl:ain thi-grea.'ler 'effect in terms of morta!tit.y of the larger burns in the ),oungergrol!lp (Pruitl,e.t,at .• 1964. PII'. 399-400).
The highercuscepti'bjliil.y to bums of very ylQl!lng children Isalso reported by Wintersche:id & Merendino (l960) and Rittenbury, Madox, Schmidt, Ha:m & Haynes (1966),
Similarly it is well known that older patients tolerate a burn wound very poorly (Moyer, [9'';4). En one large series , no patient over ,65 years with a bum. or 25: percent of the body surfacearea survived, and a- many as 18 per cent of tile older patients died with bums of oruy4 percent or tess
(Riuen'bury etai .. 1966). . .
This meansthat the youngadlJlt of military age and tandaed of tiLnes . !i . more able to with tand the phy jologica] tre ses of the severe bum than the young child or theelderl:y person . Because of the d.ifference in the age di tribution, it is dear thar a ample of the general civifianpcpulation ub~ jeeted to bums risksa greaterproportlonof deaths than a military . ample, of the same size.
[33
The limelak'en to,die
All important con ideration i:n evaluating the suffer:ing resulting from different weapon is the time taken to die. If a victim, is going to, die he will in genera] suffer les if he die immediately tlian if he die Jowliy.1ilie implicatton of the legal expres ion that weapons should not "render death inevitable"is that weapons, where they d,o not. kUl. immedia.tely., should offer the wounded persona h~gh probability of recovery ..
So many factor . are involved in different wound. that it is difficul.t to make meaningful co m pari on . However, there are indi.cation that. where adequate medical facilities a:reavaUable.. imple pelletr.ating and bla t wounds iln general appreach the above humanitarian criterion. For example, amdy .of 45094 US Army casualties iill Viet-Na:m between 1965 and 1'967 hewed tbat 5387 (U .9' per cem) were killed inaction, 623 (l A per 'cent) died of wouads, and 39107 (88. m per cent) survived. Of those wllo died of wound in hospital, 62 .. 3 percent died within the fJrrst 24 hours •. and it was concluded that a h~ghproportio," of the e ,early deaths repre ented casuahies which, in prevIous, wan with.outlUghlyeffecti.ve helieopterevacuatian, would have been classified a "killed in action". Of the wounded in action 43 . .3 per cent were returned liO dut.y within the theatre of operations within 3'0 days and 54.2 per cent were evacuated for further treatment (Whelan, Burkhalter &. Gomez. W968). These figure indicate that .. whi.le conventional weapon are by no means "perfect", neverthele s, death tend to be relatively rapid or the chance . of recovery relativelygood.
There are indication thar hum wounds, hy contra t,conform les to
ucha humanitarian criterion .. While there fs Iittle doubt that war bums have a high early mortallity, in many cases death may not ensue for days or even weeks. Ironically, the better the treatm.ent available, the more drawn-out the period of dying may be. That there is evidence to Sl!IpPOril. such a concluaion may be seen. from thelDoUowling urveys ..
FjftY~l1e girl of the Hijiyama High School in Hiroshima, Japan., were ourdoers in thechool gwund, Ie than one ki.lometre from the explo-
Table J .. 4. Day of death of .51 girlS,. al the Hiji'yam_B HJgh School, HLroshima, .!Iapan,. who r,ecehr,edsevere burusfrom the :atomJe: bomb explosion
Day allier the explosien
DaiJy death rate ofthe 51 girls
I 2 3 4 5 6 7
I'D 7 15 II 4 5 II
. ource: Ougillerson & Warren (1956).
B4
T1Ibie 3.5, Average da~ of death from burns ,In H: live-yearsuney .963-1'967) of hospitals in Melbourne, A.ustraUs"
Hospital
Number of patienl
Number of death
J\yerage lpol-bu.m dayof dying
I 2 3 4.
1'95 1.23 119 144
16 III 19 20
17 11.4 18.8 201.'9
• The Originall data includes a further 11.1 patiental four other hospitals. On'lylii:'II,e of these patients died.
Source: Ma.cl.eod (1970)'.
sioa of the atomic bomb. They were all severely burned. and lMortaIDity within one week WaS 100 per cent. However, ooly lO of the girls died OD the first da.y; the largest Dumber died on tile third day (table 3 .. 4) .. At the Kameyasaa Hospital •. aID' in Hiro b:i1ll3,peak mortality from bum, DC~ curred on the fourth day. a:JtbonghanDther peak in deaths occurred in the third and fourth weeks, when complications, including thoseassod~ ated with radiation injury. set in (Ough~ersoli1l & w.anen. ['956).
111 II recent five-year survey ·of eigh.1 hospitals in Melbourne. Australia, it was found that on a.v'ernge death from burn occurred to to 20 da.y after the lqjury. depending on the quality of •. he hospitcal treatment (see table 3.5) .. The author concluded;
T1lbl.e .3.6. Day of deadl for .5eVfnly bUToedpatinls In Sl:O(kbolm Swed~entl
ENtenl of bo{ly surface
area burned
per cent
Age 'Pot-bum:
Case }Ien!'::> Total Third degree day ofdll.ing
I. 22 100 98 1.1
2 .311 9S 90 7
3 34 '95 7:5, 20
4 60 85 80 32
5 57 80. 7'j 9
6 47 75 70 13
7 44 75 70 10
8 75 701 70 II
9 64 6~ 60' 6,
101 58: 6.5 (II)! 14
II 74 60 SO 19'
1.2 74 45 45 15
I3 79 45 40 38 .•• The original da:la include an addiliiona.l SO patients, none of whom died, All :pBtiellls. were Il'eated with the meeem warm dry air method .
Source: Birke &; Liljedahl (l97n.
135
· .... 2,0 years ago 75 % ofdealhs occurred fi"Omchockin the fir_t Ulreeday., [wherca 1
omly. the rna l eVe"ely burnt now die atthis stage although over n!cent years -
the mt.erval before deaihhas beenprol~onged. these has been little reduction in overall mortality (MacLeod. 1970. p'. 776).
Birke & Liljedahll (1'971) reported the til11.e of death f'Ora series of civilian bum. patient in Sweden (table 3.,6),. In no case did death OCiCUif in les ·.than six days,. and even for patients with a. very hiighpmbabiHt.y of dying, death was iin some cases drawn ,out to three weeks or one month. The ,(USfBrooke Army Medical Censer (1972:) reported that, for patients treated between 1965 and 1'971, the average time taken to die was 14.9 days af~e'r the bum ..
These i:ndication_ are not conclusive, bnt they are suggestive of a. significant difference between the time of deathcause<l. by conventional penetrating and blast weapcnaand thaI. caused by incendiary weapons. It has not been. po lble to trace data. in the public literature wh:ich wOldd enable a clear statement to be made on this aspect. of theproblem, and further studie .are warranted.
con equent upon severe InJury or emotional disturbauce •. reulti.ng from the relea e of hormone" nich a- adrenaline and hi tamine into the blood stream which in tum affect the nervou 'I tem; uchhock is sometimes known as .n(!umgell'ic shock. Both kinds of shock may be present in the bumc.asualty.
Hypovolemic hock is due to the los of body fluids by direct flow or by evaporation from the bumed urface .. In a severe burn. loss IQf water by evaporattce alone may amount to four to five litres per day (Roe., Kinney &: Blair. 1964). The reduction in the volume of circulating blood has profoisnd 'effects. 'on the heart and on th.e peripheral blood flow. MODerief (1966) showed that in the immed:iate post-bum period, the cardiac output of experimentallyscalded dogs was reduced to 43 per 'cent of the pre-basn level, and then further declined 10 20 per cent of the pre-bum level, unless the volume of lost fluids wa . replaced. In order to increase tbe blaodflow to th.e heart. theperiphernJ blood vessels are constricted, greatly reducing the blood _upply to other orga.RS and muscles .. Beyond criticallevels, the reduced blood flow is ill:sufficient to maruoltain the supply of oxygen to the heart muscle, and the heart fails. Cardiac arrest i: fol· lowed witihlin a. few minuees by death.
Changes in lhe electrolyte composilion,ojt'l,e body flilids
The ite.of the bum wound, where the tissue is destroyed, is surrounded by an area. of pa.rtiallinjury. In the dead tissue, elrculatian of blood ceases but in the surroundingarea there is increased permeabUity of the capillaries, leading to anincreased flow of water, electrolytes, proteins and other constttueaes from the blood into the wound, from where tbey may be lest. Thef10w .of tlquias Isindteated try seepage from the wound,
.weUi.ng of the tissue (oedema), or the formation of blister ..
It ls thus not only the volume but also the eornposino» ,of fluids 10 t that i . important ince the alts .. protein and other sebsaances whichl they contatn are e sential fnr the normal functioning of the body, Replacement fluid: ,( ee below) must contain not only large quantiUeJ. of water but aW 0 balanced amounts cfelectrolytes, the exact amount and concentration being caret:uHy judged in eaeh indivi.dual case. Nonnally water in the body flow . into thecells from theextracellular flinid by osma i~he Row through a erni-perrneable membrane from a weaker to a. stronger solubon. When water is 1.05t from the body fluids, theeoneentratiun of the solution outside the cells becomes greater than tha.t inside, and water flows ,out, leading to the death of the cells. Any fluid leak,ed from the wound will 'contain some sodium ions, and the kidneys removesome odium too, unless the concentration rises beyond the level with which the kidneys can cope i(llyperna.tr:iaemia).8 Thus the burned person may suffer losses of sodium , Hypematriaemia may also indicate increased secretion ef a'I'd:o terene, a ub lance sec-n:ledl by 'Ihead~enalglands whic'h eauses retention of sodium ions and the loss of potassium, Aldostercne :i- normally broken dawn :by the ILiver or eJlcreled in. the urine'.
Pathop:bysiology of the. su:nace burn wound
[11 thl ection the pathological effects of the bum. wound at the physiclogical level are described briefly. It is important to understand thaI a ' urface bum. is not simply a matter of damage to an unimportant area of Ute' body: not: only is the kin itself an organ of vita.l~ importance, as has been explained, butexrensjve bum wound. cause suchextreme distu:rbances that tbe whole physiological balance of the body may be up. 'et and major internal. organ uchas the kidney .' the heert and the di.ge.tive iystem threatened ..
Two specialists on bum open a major aeticle with the wor-d :
Patients withextensfve deep bumsutIer rhe greatesttrauma to which the body can be expo ed and have profound metabolic di turbance 'that perslst far into the course [oflreatm.er:lt] (Biirke & Liljedahl, 1971, p. 5).
These gener.al metabolic d'ect are tbe primary initialcau e . of death, and present the immediate ,chaUellge for treatment
.. Physi%g.ical chan.ges ill the shock phase
The initial phase following a burn wound is usually known as the 'shock pha e'.' Shock here refer to hypovolemic., or oligt:I€,nichock, iii physiological yndrome re ulting from a reduction in [he volume of blood. It bould be dis tingui hed fm.ffl the profound mental and nervou effects
7 The many use. of the term shock make il: un uitable :for scientific u e. Howeverv the term is still widely used! clinically lind 0 il. is u ed here. Simeone ('1963) reviews the hisl.ory of Ihe term and attempt !O combine semantic clarity wil.h physiological complexity ,
ions from the ti ue > even though there may be a higher concentration in the (reduced volume of) bod.y fluids ..
The balance of potas iumion is affected mewbat differently .. Potas-
ium is normally f und in a higher concentration in the Intracellular fluid rather than in the exrraceflular fluid. Whelll the cell are destrcyed by heat or by dis ea e , additional pota ium ion are relea edinto the body fluid '., Thu there may be an initiairi e in the concentration of pota ium ion hyperkalaemia) following a bum. If the kidney continue to function normally they will remove orne of thi additional pota ium 0 that, a the ti ues are recon tituted, there may later arise a condition of hypokalaemia due to a hortage of potas iurn ion. In the fir t day or two of treatment .it .i uuaUy unnece a:ry to replace lost potassium ion (PhilUp & Co table undated), but careful monitoring of electrolyte concentrationsin the b dy fluid: remain, nece ary for some time to avoid hortage later. (Table 3.1 record one death from hyperkalaemia, and four from hypokalaernla.)
han e in blood protein level
The major component of the blood are pia ma---a fluid which contain dis solved alts, protein (such a albumins. globulin and fibrinogen) and other comp unds-red blood corpuscles, containing the red iren-ri h protei.n haemoglobin. and white corpuscles, who e principal function i to protect the body again t the invasion of microorgani m .
Extensive deep bum m,ay re ult in the 10 of a much as 20 per cent, of the red c rpu de iljedahl, 1967). The red bl dell are broken down, a proce known a haemoly is, releasing the haemoglobin into the plasma (a condition known a· haernoglobinaemia), from which it may be extracted and e excreted in the urine (a conditi n kn wn as haernogl binuri.a.) ... Removal of red corpu de from [he circulating bloe d may al result from local thrombo i -the formation of a cl t of blood which occlude a blood 'lie sel-in and around the area of burned ti sue .. Damage to. the capillarie in non-burned area a a re ult of thrombo i ha been demon trated e perirnentally by Artur on (196]) and y Birke and h:i colleagues (960).
In addition to the 10 f blo d protein by direct flow from the wound
and by haemoly i , there are other large fluctuation in thelevel , of blood prot in , which appear to be related to change at the ite of the wound and to the greatly increased metabolic need of the burned per on, Since it i difficult toupply ufficient additional energy from eternal ource the body turn to meta lizing it wn protein. The re ult i a evere initial decrease in the blood protein levels, which iln evere bum may be r duced to one-half of normal level (Liljedahl, 1967 . Sub equently, mill - de ti ue i . metabolized, and the patient' weight decline rapidly.althougb the blood protein level return to. normal.
138
Chan es in the kidney function
The kidney have two. major functions. They pltay a major role in maintaining the water balance of the body. Se ndly, they e tract a range f waste products from the blood and pa them int the urine which i thenexcreted. The kidney con i t of large number of tubule. In the fir t part of each tubule, kn wn a the glomerulu , water and wa te PI1 ducts are filtered 'Ollt of the circulating blood, In dl;e la t part ofthe tubule some water is reab orbed into the blo d while the waste products and the remaini,og water are pa ed into the bladder urine. The e proce es are
reguts ted by hormone uch a tho' produced by the adrenal gland
djacent t the kidney.
The decrease in the volume of the circulating blood, due to los from the bum wound. h emoly is and thromboi induce con triction of the blood 'lie el which further decreases the flow of blood through the kidney . In the initial po tbum pha e, the flow f fluid through the kidney may decrease by 30-50 percent. The amount of fluid filtered by the glomeruli i reduced by 40'-50 per cent, while the re orption of water in the tubule increa e the b dyatternpt to maintain the fluid b lance. The higher concentration of wa ite products may block the fdtering action of the tubule • hindering the excretion of waste product int the urine.
he frequency of confirmed kidney damage resulting from larger burn wound varie between 9 and 12 per cent in varioutudie (Liljedahl. 1967). Electrical and exten ive pulmonary bum are particularly liable t produce phy iol gical di turbance ufficient to. re uH. in renal. damage (Birke, Liljedahl & Linderholm. 1958; Birke & .. iljedahl, ]966). Kidney damage in patient witbe ten ive bum. greatlyc mplicate the progno i . even where an artificial kidney i available. Mortality in the e case i high (Cameron,1969).
Damage to the dige tive ystem
During the initial phase of the bum injury the muscle wan f the inte tine may be paraly ed, sus pending peri tal. i , the normal wa e of alternate contraction and relaxation which cause the content of the alimentary tract t be propelled forward. Tbi may be followed by acute retention of food in the tornach, Change in the gatro-inte tinal tra t Im3Y cause ulcer _, indicated by vomiting of blood and the pa age of dark. tarry-col-
ured tool, due to the presence of blood chemically altered by the inte tined juice . (melaena]. Gastric and duodenal: ulcers an e in orne ca e . in t:he surf e and in other. a deep, acute ulcer kn wn a Curling' ulcer . The e ulcer may re ult in dangerou haemorrhage and perforation . The pathogene i of uch ulcers i not fully ascertained although the rna t widely accepted hypothe e include the effect. of hi tamine. teroids, hock, ga tric acid, rnicruemboli and endotoxin. a po ible causa-
139
tive agents (Pri en. 1950; Moncrief, Switzer & Teplltz, 1964.; O'Neill. Pruitt & Moncrief 1968),
Even in later phase: of the bum iQjury, particularly wh re chroni infection of the wound develop, difficuhiesir; dige tion may reate pr blern in maintaining an adequate IUlltriliomd tate.
Changes in {he hormone balance
The physiological tre due t thermal injury timulates the production ofa number of hormones. particularly those produced by the adrenal glaad (Biirkeel al .. 1958.; Feller, 1962).
Adrenaline. al 0 known a epinephrine, i released by the medulla of the adrenal glands and timulate the heart inhibits the movement of muscle wall of the inte tine • relaxes the bronchiole of the lungs and c n-
triers or dilate the blood vessels. NOli3drenali.neec!retioni· 311 0 increased; this hormone pm e e tbe excitatory function of adrenaline but not the inhibitory function. The production of cortico teroid hormone by the adrenal gland also increa e .
In me case, however, the tre of thermal injury re ult in haemor-
rhage and aecro i. of the adrenal glands. whichin tum lead to a lack of adrenal hormone uHicient to cau e death (Foley .Pruitt, Myer & MOIlcrief 1967).
In the first hours after the wound occurs there is a large increase in the concentration of histamine in the blood. Hi tamine is a hormone which i , Uberatedas a, re uli. of injury. It causes itdil:i,ng or pain, dilation of [he blood ve els, reddening of the kin, lowered blood pre ure, increased ga tric ecretion and may result. in shock-like manifestations. The liberation f large quantitie of histamine into the blood may be a po sible contributing factor to ga tric ulcer, and to the general capillary damage evidenced inexten ive bum, njljedahl, 1967). Heparin Ita been used experi mentally in the treatment of burns becau e of it tr ng anti-histamine effect. Heparin appear to decrea e the ize of the burn, horten th healing time, and ignificantly relieve the pain (Saliba, 1970; Saliba & Griner. ]970), although its use cannot be prolonged in e it interfere with the blood-clotting meehani m.
The problem of hear loss
One of the major functions f the kin i to prevent the evaporation of the body fluids and the 10 of heat. from the body ... Apart from the threat of hypovolemic hock due to 1.0 of fluid _. the evaporation of each litre of water require 580 kilocalories of heat the latent heat of vaporizatlc n of water). Figure 3.5 bow that the rate of evaporation of water for varying areas of burn wound may amount to many litre per day, compared with the rate frcm the uahurned body urface. In an. attempt to maintain the normal. temperature of the body, the everely burned per on u es up large amounts
140
86 per cent totall, . __ . BO per cent third
degree bum
___ ,30 per cent total, 23 per cent third degree· burn
25 eerce nt lot.al,
o per cent third degree bum
W,///h Normal rate W//;~ of evaporation
Figure 3.5. Rate of evaporation. of water In three patients wUb 8S 30 and 25 per cent burn wounds compared with normal valu _, durfng rtr t four weeks after
Irtjury
ml/hr 200
180 160
140 \,
120
100
OL-~~ __ ~~~~~~~----~~~~
2 4 6 8 10 12 14 16 18 20 22 24 26 28
ource: :LiljedahII19TlJ,
days
of energy .ome calculati n of typical energy requirements are given in table 3.7. It will be een that the verely burned per on may u e up to twice a much energy a normal ju t to compensate for the 10 . f heat by evaporation of water.
Theincrease in the ba al metabolic rate as a re ult of burn w und was reported by C pe, Nathan n, Rourke & Wil on (1943). Birke et al, 19 8) hawed that the ba aJ metabolic rate may increase by a much a 100 per cent several weeks after the injury. Thi increased rate of metablism
Table 3.7. Aerage daily rate of evaporation of water from bum woun~ or arying extent and corresponding heat 10 due to fhl eaporation compared With the rate of wa.ter eva,poratJonfrom a normal :llduU male
rea of 'third degree burn per cent
, oss of water by evaporation /irTes/day
20-4fJ 40-60 60-90
1-2 3-4 5":7
ormal 70 kg male
approx. 0.8 .
ormaJ 70 kg male
basal heat pr duction moderate activity
a The. latent heat of vllponiza.tion of water i 580 k:ilocalorie ource: iljedahl (1971).
Heat. .10 I dueto evap ralionG kilocalories /day
·80-1 160 .1. 740.-2 320 2900-4060
14J
pre ent a major pr bJem in treatmentv since the ever Iy burned per on, who frequently devel p .. cornplieati n in the digestive tract ha great difficulty 3'imi[ating ufilii:cient qua:ntil.ie .of nutrient to provide 0 much energy.
Where nly imple rnedi al facilitie are available II I a comm n e - perience that tbe everely burned per on in fact u e up energy fa ter than he i able t replace it from food and a a re ult 10 e weight rapidly. Gestewitz (1968). for example report that for bum patient in North Viet-Nam, weight 10 e may be a much a I kg per day and finally average a 10 of I: per cent f the normal body weight. Thi: remarkable weight 1 gav ri e to the e pre i n "napalm int xification" and i very difficult to cope with e cept in the most advanced treatment centres," Roe et (1/. (1.964, hewed that lowing down the rate of evaporation de rea ed the heat 10 and lowered the rate of rnetaboli m; thi finding led to the method reported by Liljedahl (19 7 whereby warm. dry air i pumped into the room in which the patienti treated. Thi increases the rate of vaporation temp rarily, but the wound r-apidly drie . and after two day the rate of evap ration, nd hence the increa ed rate f ba 1 metabolism, decline COil iderably.
Pathophysiology of "pulmonary burns"
Inaddition to the urface bum de cribed above, fire may cause death or injury by . ariou form of damage to the lung and re piratory pa -
age . The e injurie are often referred t a . 'pulmonary burn ". Such 'bum ., have; now been re ognized a one of the principal cause of death by fire (cf.Phillip & Cope 1962: Shook, MacMillan & Alterneier 1968).
It wa at fir t a surned thet the victim of pulmonary burn actually
uffered bum of the respiratory tract. and the lung . due t ,the inhalation ,of flame and hot air. It i ow realized that the term i omething of a mi norner: thermal injury of the lower re piratory tract i rare, ince the flame. do n t pa beyond the no e and thr at. and the heat of the air israpidly di iip.ated efore reaching the lung. 'Only where : tearni inhaled doesthermal damage to the lung p ibly occur, . ince team ha a thermal capacity 4000 time great r than that of dry if (Moritz. Henrique & M Lean, 1945}.
However. there is no doubt that pulmonary complications are a ignificant cau e of death. In many ca e . pulm nary complication, ari e a direct equel to bum of the face. 110. mouth and throat. or theinhala-
• H rn 11969) g.i es c i id account of such a problem in the People' Republi of hina: .. ! u time when he most needed nourishment. the patient' appetue started to flag ... 'i hen Ihi newsleaked oul the chef of'. hanghai" famous restaurantsput their heads 1.0- gether , .. and sent a stream of delicacies 10 (he hospltal , .. " (p. 10 ). Ironi ally. [he
• m wer is not tempting dishes but the iniravenou admini tration or an emulsion of oybean oil and egg. yolk. tee below. page 169J.
142
Table 3.8.. Major cause of d alb in 38 patients woo died - II result or InllalaUon injury"
umber or patients who died
Pneumonia 1.5
iLarYUSOllfachcobronchili . 8
Bum wound sep i~ 6
Re piratory tract burn
Pulm nary edema 2
A.lelecta i
Myocardial infarction
Cardiac t rnponade
Ga trointe tinal haem rrhage
Tollil 38,
• The data are gathered from the h spital ~ecQrd- oflhe 2-97 patients treated for !berm~ injurie· at the US rmy In titute for urgical Re earch between 1956 and 1968. Sixty- I patient were identified with inhalation injur • and of these 3 died.
ource: DiVic.enti, Pruitt & Reckl:er (:1971.).
tion of large amount of srn ke r fumes, particularly in a do ed pace. W,JiJJlilethe majority . f such injurie occur in confined pace, one tudy
f 66 patientsshowed that eight patient u rained moke inhalation injury fr m accident that occurred in open area (Di'Vicenti, Pruitt & Reckler, 1971.). Mortality in the e ca e i very high. 'Of the 66 patient mentioned above. 38 died. a mortality of57.6 per cent, Thi may be compared with an
v rail mortality of 9.6 per cent for thermal injurie treated at the arne in titution in the la t year of the tudy, The major cau e of death in these patients are shown in table 3.8.
However, pulm nary complication frequently ac rnpany bum injurie even where imrnedi reign f inhalation injury are n t vi u . A 20-year uJ'veyat the Ma aehu 'en General Ho piral showed that ;88 per cern f burn patients developed respirat ry c rnplication (Phillip & Cope, (962).10
Pul:monary complicati n take' a number of forms • [he most. important f which are inhalation injurie due to make and to ic fume • pneumonia and pulmonary oedema.
Inhalation injury re ulting from m ke and to icproduct of combustion i characterized by evere inflammation of the trachea and bronchi due t the chemical irritation of the mu ou membrane lining the e re piratory pa age. Thisinflamrnation may lead tc severe breathing dim ulties, Clinical indications include the pre ence of carbon particles in the putum wheezing, hoar ene and coughing. triking change may be vi ible n a che st X-r y. The patient with inhalation injury i particularly us c.eptible to bacterial mfeetion of the tracheobronchial tree (Pruitt et al., 1'970),.
eu Thi institution did n t u e mafenide acetate cream. which may lead I additl n I re piratory complications. See page 1176.
143
Suchinluriesere similar to those caused by the type of cllemi:cal warfare agent known a the lung irritant ( ee chapter 4).
Pulmonary oedema m t commonly occur in patients with large bum, e pecially children and older patients, patient with a - - ociated renal failure, and patient to whom inappropriate amount of fluid were admini - tered at the, time of operation performed in their po tburn period (Pruitt et al., 1970). Mortality in the e case is high, althoughit may be accounted for by the large average i ize of the bum and other as ociated factor . A potentially fatal lung edema may occur with con iderable rapidity even quite late in th recovery peri d (Walder et al., 1967). Thi in tum may lead to a weakening of the heart and decrea ed blo d circulation. Continuou monitoring of blood pres ure and blood volume is required 0 that. if necessary, early mea ure can be taken to prevent decreased btood pressure leading to irrever ible ti ue damage of the heart and other organs.
Pneumonia ia dise e of thelungs resulting from infection by bacteria.
The bum wound itself acts as a medium for the culture of bacteria which maysubsequently infiecttbe hmg . either through tbe blood or through the air. In one Judy of 70 burned patieru . who developed pneumomait wa found that 23 (33 per cent) were infected by airborne bacteria. while 47 (67 per cent) were infected through the blood. In a ubsequent analy i of 113 patients who were treated with an antibiotic agent it was found that 74 (65 per cent) developed pneumonia from airborne bacteria and 39 (35 per cent) from bacteria in the blood. Nine (13 per cent) of the patient in th fir t group, and 25 (22 per cent) in the econd group, died (Pruitt. DiVi.centi , Ma on, Foley & F1.emma,I970).
The problem of lnfection
In pile of many recent advance in medicine, the prevention and treatment of infection-c-entering the. body through wound from whatever cau e=remain a problem of great magnitude, Where advanced medica) facilitie are available, enabling ucces ful control of the hypovolemic shock pha e, infectioni generally the major cau e of death following bum.
The deep bum i an id aI . ite for infection (Artz. 1964). The m isture and warmth of the body provide a near perfect medium for the growth of a range of bacteria. which find abundant nutritive material in the dead ti ue and multiply rapidly. Thrornbo i and 0 dernain the ti sue deere e the fl w of blood and thereby inhibit the patient' natural defence rnechani ms again t bacterial inva ion. P r the e rea ns, all deep bums becom infected to 3. greater or leer degree. A large bum wound may contain thou and of gram of highly infected ti .sue, and organisms from thi lis ue may enter the bl od tream or be breathed in by the patient, cau mg generalized infection, or epticaernia .. When infection reache thi tage
144
• ... he everity of a cutan U' bum wound depend not only upon t~e depth Of. the burn but al 0 upon the extent of the body surface area .affeclicd. w:hl h de~erml~e the los •. ofbody fluid" and heat, and therefore the impact n the major phYclologlcal
y tern. of the body." (p. 126)
"There i a direct relation hip etween the extent of a bum of a given depth and the chance of urv i al." p. 12 IT)
"While there j linle d ubt thatar urn ha e a high immediate mortality, in many ca es death may not ensue for day' or even week. ,. (1" •. 134)
10-743168
"The everly bumed person, who frequently develop c:omplicatio~ in the dige tive tract.ha- great dlffic:ullyas-imilatins ufficient q~antitieof nutrients (p. 142) .. : Since it is difficult to upply sufficient additionaltenergy from eternal source . th body turn to metabolizing it own proteins . .. and the pati.ent' weight decline rapidly .. .' (1" 138)
"There i no. doubt t~at pulmonary complication are a. significant cause of death. In many ca es. pulmonary complication an e a a direct· equelte bum of the face, no e, mouth and throat. or tJhe' inhalation of large amount of mokeor fume, particularly in a clo ed pace ... H. wever. pulmonary complication frequently accompany burn injurie . e en wher immediate igns of inhalation injury are not obvieu ." (p. 142 fl)
"Where there are igns of Lipper re piratory tract ob truction, large am unt of liquid in the re piratory pa age or hallow breathing.tra heotomy=the operati n of making an opening directly in the trachea ('windpipe') 0 that oxygen may be admini tered bytube-s-may be required. Thi hould only be done; where it i clearly warranted by the ob erved ymptom •. ine tracheotomy may be itself a factor in pulmonary infection." (p. 171)
"8urn frorn napalm rno t typically OCCur n the unclothed a:rea of the bod . pa.rlicularl!y 'the hand_.head and face, and feel: and leg. Becau e of the thin layer of tis ue Over the areas napalm bum rapidly affect the underlying mu les, tendon and bone which greatly compli ale, the urgieal problem. Recon tru ti e surgery t treat uch condition require a I ng erie" of Operation' 0 er se eral year and is unlike! I. be available to rdina pe pi ill mot ocietie - in artirne COndin a .: (p, 154)
"Hypertrophie scar is ... thickened, raj eel ami grate que ... K.eloid ... may progres sivelyextend beyond the site of the originaltrauma , .. kin cancer i much more prone to develop in car cau ed by burn than in normal kin." [p, 146fj)
"AIl full thickne burn heal with
ome degree of car ... •• (p. 146)
"Contracture ufficient to cau se eriou functional di ability frequently OCCUr in the case of deep burn w unds or the handand the head and neck ... Burns in the e location are particularly common in the military conte r." (p. 147)
the chances of survival are not. great, According to Moncrief & Teplitz (1964) over SOper cent of late death fonowing bum result from epticaemia.
Large bum wounds are particularly pr ne to infection becau e of the e tent of necrotic tissue. Infection of clean mechanical wound, for example tho e ,re ulting from low velocity bullet, i relatively ea y to contain. The bullet itself. or pie es of clothing or dirt carried into the wound. may infect it, but the area affected is generally restricted to the Immediate vicinity of the bullet path. Dum-dum bullet and very high vela ity bullets on the other hand. cau e an "exp!o ive-type' wound, where ti ue i damaged at a considerable di tance from the point of c ntact with the projectile i elf; and this type i much more liable to ec me infe ted due to the much greater volume of necrotic ti ue acting a: a. culture medium for infective bacteria. Given that in general there i a direct relation hip between the size of an open wound and the amount of infective bacteria which grow, it i . obvious thatthere are very large quantitative increa esin the amount of infection resulting from the entry wound of a bullet. whichi less than one squarecenfimetre in area the exit wound ofa high velocity bullet, which may be many square centimetres in area, and a bum wound which may. potentially, cover the total body area of approximately 1.5- 2.0 square metres.
The nature of bacterial infection i highly dependent upon the circum-
tance and geographical location of the patient. In heavily populated and highly cultivated area the likeUhood of infection from grit and dirt in wounds is greater. a major factor to con ider in combat condition . A World War n tudy of the bacterial infection of comparable wound showed that only 30 per cent. of wound incurred in the Libyan de en were infected with Clostridium welchii, wherea in. France 80 per cent were so infected (McLennan, cited in Cope, 1953. p.IS).
The development and utilizati n of new antimicrobial agents during the pa t 30 years have resulted in change in the type of rganism repon. ible fur fatal] infection of bum patient . Streptococcal and taphylococeal
epticaernia predominated prior t the availability of antibacterial agents effective against thee organi m . Since the late 1950 . other organi illS •. predominantly Pseudomonos a eruginosa, have emerged a the principal offender (Pruitt & Curreri, 1971).
Thus, the exact nature of the bacI,eriall infection depends very much upon the circum tance in which a particular patient find him elf, including the type of treatment available. Whatever the cause of infection. however, bum patients. tend to be particul.arly usceptlble, Thi i due to the other effects of the bum on the body, including an initial 10 of circulating antibodies and decreased ability of whire bto d corpuscle to kiU bacteria. repre entinga decline in all f the body' normal defence mechanisrn again t infection Liljedahl, 1967).
11-143168
145
DlsabiUtJesresu]tlng from burns
Severe bum wounds usually resuh in di ability even art,er the w und has healed ..
The disabi:lity following the healing of the bum i due to a number of faclor ... The rno ! common .one . are d.i. abiUties due 10 car iiol':m'alioll,. to the development of kel'old~. ~o, c:ontractu~es in ge.neraJ, to lowered resitan.ce to oLiller di eases, to pychic trauma, to tile de\lel'oJPmellt of unwanted emotional eomplexe , to inabiliiyto as-
umeformeli to.leinoc:iety, and theloss ,of strength and activity (.AI~dric:h.I941, p.581).
Sca_rnQg eccurs when the bum invoWves the fiwdW ~hicknes of the skin and underlying tissues .. AJl full! thickness bums heal w~th some degree of
car ... SkillgJafts, .. if used, never perfectly match the adjacent skill and are surrounded wiena rim of scar, espec.ial~y if grafting Is delayed! or if En. fecti.on prevents prompt healiilQg of the bum. Ilill a large bumthesewreas of sear are very ext,ensive and eon picllIous.
Thi scarred tissue may develop a. number of abnormalities. Hypertrophic scar is defined as "a. pmk, whit,e. or td'a.Qgtiect.aticll scar w.hicb is hard, taut, unyieMjng, and more or less fixed to deep' tlssues' (Wells & Tsuldfuji, ]952. p .. 130). Although they may be thickened, raised and gmte que, they do not normally eX.t'endinto' undamaged skin, and if ten. sica is reduced by r,e.lea.singcontracture, or if adequate'kin grafts. are app.lj,ed, over the course of tlme they general!l)! . often and become much thinner .. K'eloidis a term introduced by Alibe.11 j'll: 1806 and has been detilll.ed as "a. l1lovable,supemcialle ion. presenting an exuberant Jobula[,ed, overhanwng profile, a. gli tenins, jnJ]!amed or acrocy.anoticll surface,. a rub~ bery censissency, andlchar.acteriz,edymptoma.tkally by a pricldy, burning it,eh", (,bid .), Keloid are cumulenve rna ses of cal' tissue that may pro-
. gresslve]y extend beyond the site of the original traurea; ,character.i tleaUy, if keloidsare ,e.xci ed, a larger keloid results. There ws therdlnean impo.ttantsurgical distWrlct[on between the e two types of scar ,. although ".diiffIculties i!n c1inicaJ interpretation canan e whelill one approaches the: other inappear:ance or when the twoexlr,emes coexi t In the same patient" (Ibid.).. In addition there ma.}! be scarring whicb presents: a raj ed or irregular surfa"ce"or a thlekness greater tban the surrounding normal skin, which is somewhatdi:tferent again from kel,oid Or hypertrophic. carri~as defined above ..
It Is generally agreed that the incidence of such abnormal scarring depends upon th.e . 'ev,e.nr.y of the initiall injuf)',tne madequacy 0.1 early treatment, the incidence .of infection. and delays In .heaLing due '0 mal ...
II. l~/Q~flgieC'taSi~ (from ~~~ ?reek 11!1.0s.e~d; aggeiQ!I,ves el: eklo£is, exten iO!l) lis the dlla~lQn. of 8l'OUps?i c-apilJanes: iorm!l1,g rn.!setil'. dark red, wart.like growth5;acmcyanQ.tic ([romlne. Greek.a/(ron, exll\emJ.ly; k)lOIlO~i$, dark blue colour) mean dIscolouredl blue or dark pll.l:pleatlhe. finger tips or OIherex.lr,emities, due' to the presenee ,of abnormal amo~!ll
of reduced haemoglobin, in the blood. - .. - -
146
aurritien or absence ,of -kin-graftillgand other factor ,(B~ock & ! 'III~uk~. 1948: Wells & Tsuk.ifliji., (952)" Such factors may ,explallil the Ill1gh mcidence of kel.oids fbllowing the incelildiary and atomic bomb attacks on Japan, .althougb some author. suggest that racial! characl.eri. tics may also be iin.vol.ve.d.
A • econdary factor is the known dispoi[ion for kel~idformalio~t? occur among t.he: Japene e and ot:i1er clark- killnedpe pleas a racial cheracteristic. Many spe~tacular keloids, for example. were formed after the heal.ing of bum . produce~ III the incendiary bomb attack on Tokyo (US Depa:ttm.enl,of Defense, 1.962.p. 70).
Keloid • wbich are extremely rare in. the patient po.pul:ations typical of most of the present-day medical literature, have been. noted in Vi.et~ Namese bum vicllm_. by Liljedahl (l90n and Con table (1973).
wen & Tsukifujw 0952) noted a [iendency fo.r abnormal scar to disappear over a period of year.c unle provoked by illfecli~n,fo~eigo bodies, suchas retained fragments, contractures or abnonnal skin tension.
Coutractures are due to the: restriction of undedymg; muscle and joiRt . bysuperi:mpos·ed carol' inadequ.ate grafts ... Contracmre bandsof fibrobfastie ceUs are formed in the gran:llIlation tissue that builds up in 'the burned areas. Thee centracture band may be very dense and. can produce mall.), untoward results, Conliractur;es suffic:ient: to cause erious functional disability frequently occur in thecase of deep bum wound ·of the hand and the head and neck, wbere they maycause hideous deformity. Bums i~th~~e locations are paeticularly common in the mmtary context (table 3.'9),
D.isabilUie uch a centraetures and keloid, may nOI: develop until
week or month, after the wound ha healed .
If uch cli abilities inrerfere with the movements of the body" it is impossible for the individual to a um.eall of hi former functi .. ons and dutie . FrequenUy.contracture ~a~ occur arounderiflees of the body pr~venti.ng or inl,eriiering with. natural fun.ctians such as defecation. urinationr. sexual interceurse and eveneau'n.~. L:u.e. dls~ abil.ities are prone to produce a lack. of ociall adj,1I tment, UlIII havlfIga dl.reci bearing 011 [he emeticnal stability.of the patient (A:ldric:b,1943. p' .. 582) ...
Such complication demand a. long erie of recoastruetive urgical operations coupled withphysio- and eccupational Ihe:rapy in. order to produce a functional result. Thi proce __ .,pr:ead over many mnnth or even year .. is both painftd and stres ing- to thepatient, It places gre~u demand 01:1. hospita.11 facilities. Asa resultadeqaate treatment may only be a~ai,lable to tho. e able to call upon con iderable economic reaourceaandi lea t
likely to be a vailable to' tho' e rna t.prone to such complication . . ...
Further i:1 is at well established fact that skia cancer i . much more bable to dev~lo~, in scars cain ed by bum than in nor:rnal.kin (~ang,.1925:
Johnson, ]92,6; Treve &. Pack, 1930; Lawrence. 1952).. There I • evideece that this is even more likely to. occur where bum wounds have Dot been
147
n tper celli)
Read Upper Lower urnberot'
and b- extrerni- extrernl- Geni- wound, umber of
Wounding: agent nCl;;k Thorax demen lalia, per ~genl patients
BUlliS" 21,2 lJ.3 7.J 36,1 7,6 7,6 224
Small arm 10.2 /2.8 II
9.8 25.8 38.6 1.11' I 093 82
Mon:ar 16.1 15.6 6,9'
Mfn,e 25.6 ,]2.1 1.3 II 728 1 170
/7.7 10.0 6.8 263 ]5,8 1,2 I 061) 661)'
PUnji slake< 0.0 0.0 1.0 9.0 85.0 3.0
Native" us Il.B 65 6.5
1.0 34.0 36.0 1.0 68 44
Other" 275 19.4
5.5 26.4 35.6 5..6 ,I 339 I 014
All WOUJlds /5.7 /1.2 7./ 26.1 34.8 3.9 57, 3953
Normall per cent
body slJrface 9.0 l8.0 .18.0 UW 36.0 I,D' ~1 . .JIle39~_pa:ljent5in :thL ~urY~y were~ou~d~d i~, II, total of.5 (7 bodyr,egion. dIal is, an average of ~ oF~ ~lIenL The d~la do ,001 Include killed IfI {J('II~n, •. becau e I~I calegolj'is not brought 1(1 ho pitals, e A. fire~';:8burns pallenu'68 £57.7 per cenl)were ~ICII,msofacc!de,~I,' ral;he!' than ofhostiJe action. . and heav rdlelnh~d'_ s~3.!pe~e~ bl amboo fak~ -, concealed 111 foliage. which :readily penetrates cnrnhat boots · ---, ~II}' co . mg. IQJ!.!ryUlg, ow,er ,clCtremllle. .._ - .
: "Natlve_" ~~r~rs !~ i1ijuries reo uhing from ueh weaaons asarrows and pikes.
w~e/~:f .. ~th:r~at~gory II'Ic!udes 398 non.~alt!e inj~red patient ;. the remainder include patients · c~ e bl Y ~npec'l1ied mech!!msm :uc~a~ kmfi"cgn,.phos:phorus grenade. home-made bombs blas;
InJunes, unl traurnavar ol.herwte uncla Ifred type Incldent.s" ,
Source: Kovaric. Aaby, Hamil & Hardaway (1969).
gr-all.ed. ae an early tage, when il may well be that, in tead of healing, [he wound becomes ulcerou for a period of month or year. before becomin~ cancer~u ., Lawrence 1952) record I W such case, with period of ulceration rangtng from 4 month. to 61 year ., The latent period beforethe on ft. of cancer may be: many year andis inver. el:y correlated to the age of thepe on at the time of bum injury. For example, a per on burned in childho d may uffer from a caneerou growth of the car when he is 40 or 50 year .'~I~. TId' kind of complicatioll.i now rare where modern treat-
ment facilities are available but may be more 'freqll'ent· wh e ,'I.. ,I': . "'.1'
· . - . '. . •. ' " . . .... '" '.", , re' lICllID ~aC'I.I-
~le. ar~?ot available, fior ,exa.mplein uaderdeveloped countries. or ill. mdust(,lsll!zed countrie , fol'lowing mas destruction.
A'~djt~onal ~Io~,g~ter.m patb?phy iologicall! problem re ult from the .effect . of hock. and 1IIIlfectl0l1, which may affect the kidney· liver h" 11· nd
[ . .. -, "ea ,an
un~s,~esul'ting ina ~ermanent weakening of the individual!' ability to
resls.t dll ea ,e, and facmg the victim of eriol! bums with a. further intermediate ,andlong.:term .haza.rd, Renal compllcarioes, such as nephriti·. may have a permanent nlfluence on the heallh oCllle patient and hi life ~xpe,ctucy, Prolonge~! Infecncn which il!lilJre the head may force the pa,t~ lent Into a. sedentary htie.
1~48
Ps¥cbological effeets of burns
The .immediate psychic impact of the bum wouad may 'be fnllowed by intermediate a'Rdlong~ter:m p ychologkal effect on the patient
A number of faetorseontribure to a verysevere psychological burden on the burned person (Hamburg, Artz, R.,e.i , Am pacher & Chambers, 195,.3; Hamburg. Hamburg & de Goza, 1'9-3). The event it elf, due to the relalivel:y I ng time invclved in inflicti'ng a bum compared with. say, a bullet wound is likely lo have been particularly traumatic .. Extern ive econd degree bum. where the nerve ending are band but. not de troyed,.are excruciasingly paioful, and may give rl e to profound mentaland phyiesll disturbances .
The problem of combating palin andiafection may themselve create psychiatric problem :for the patient Easing pain by theadmiai tration .of analge ics Delli a morphine may create drug-deperrdency, and withdrawal from thee drugs maycause additional painand distres . Topical treatment with iliv,er nitrate" to prevent infection cause tbe h.ealthy kin to tum black: thougil'll this is temporary it may be an additional eurce of anxiety fOr thepat1i,enl and relatives ..
Pad:icuhurl.y In the case of a child, lhepa.t~ent who is isolatedand receiving only occasional vi its by masked and robed hospitaJtaft' mustalso
cope with re u[tingemoliona] problem r ;
Wi,th ome trepidation we havepermitted nurses on our Children's Bum Service to work unmasked. The p yehologieal effect of rna-ked attendent- i unde irable, and [hu far we have observed noevidence 'of a deleteriou effecl 'on the wound'" by having thenurse unmasked (P.hil.lip &. Constable .. undated),
The psychological problem of isolation L exacerbated by the more
opbistic.ated treatment facilitie and i most extreme where the patient is completeliyisolated and observed bytelevisi . en 'cameras and remote rneasuring intfument, he emotional-train of having to conlront alone the sight of one' own naked and burned body Iyin:g ona bareplasdc beJCI, andthe stench of one's own rotting fle h, cb erved only by t.hecold eye efthetelevi .ion camera,. i . difficult for the ulililnitiat,ed to envisage."
In many underdeveloped countrie It i cammon for' the patient to be attended by hi family. thereby gaining considerably in pcychoIogica:1 rea urance and emotional . upport-e-factcrs which may be overlooked in advanced industrial societies. On the ather hand. [he limited method of treatment availablatothe bum patient lin most underdeveloped eountries greatly dirnini 11 the pro pects of recovery, thereby muhiplyingahe attendant emotional strain that this impli.es,
Thesum of the p -ychiatriceffe·ct" upon the everely burned may be
II See page 1.76.
13 'the emotional 'strain on the altending 'personnel: isal 0 enermou ' and even experienced medicalpersonnel have been known 10 ask for Iran fer" from burn unit.
149
overwhelming. At be t, the patient with extensive bum will be seriou Iy scarred in pite of all effort at reconstructive surgery. Many of th se disfigured patient , even in cat e where 6unction ha been re tored, will p ychologicall.y withdraw and never make an adequate ecialreadiu tmenl.
It j an unfortunate fact that little can be done to ease the p ychological problem since it is to a large degree a function f the emotional hock elicited among the ocial contact of the patient by hi! evere di 6gur·ement, Burned per an may find them elve ociaUy tigmatized a in the case of the _ urvivor of the atomic bomb attack on Japan, wh e keloid deformitie re ulling from burn rather than radiation mark them a . Mbakusha, a. name connoting di ease, defect and di grace (Lifton. 1967).
Hl. Casualty effects of incendiary weapons
In thi secti n a description of the known effect of incendiary weapon i given. In th.i connection it hould be borne in mind that the. pecifie ef~ fects of incendiary weapon depend up n the circum taace of u e, the quantity and type of agent u ed, and factor in the target population uch a age. general: health and nutritional tatus, degree of protection, and medica] fa ilitie available ..
Metal incendiuy burn
The metal ineend:iarie . are characterized by high burning temperature and the tendency to splatter mall particles. of molten or burning metal on the victim. These s mall particle may cause mall but deep bum . Such burns are rare in civilian Jffe; they normally occur only among workers in munition factories and among per ions • ubJected to. incendiary bombing (Artz & Moncrief 1969).
Magnesium bum- produce ulcer which are mall at fir t but which gradually enlarge to form extensive le ion. According to Wil on & Egeberg (1942 the deeper part of the Ie ion i usually quite irliegllliar. Tis ue destruction may be increa ed by the formation of mall bubbles of hydrogen in the wound (US Army, 1968). The outer layer of the kin must be craped under Iocalanae the ia soon after i:njury in order to remove the magnesium. However. depending 00 the ize of the particle • magne ium may form a rapid or a slow burning ember. If the larger slow-burning particle penetrate deeper than the uterlayer of the kin they mu t be thoroughly exci ed urgically (Artz & Moncrief, 1969).
Burning thermite produce particle of iron which at the temperature of combu tion are molten. Thu , while not actually burning, the drops f molteniron are capable of causing small, deep burn until they cool and olidify. The e particle . mll t then be surgically removed. In practice the
~50
hestand flame. from thermite clo e. enough to bed drops of molten iron n a victim would probably have greater clinical effect. causing evere burns or death from hyperthermia.
Napalm. burns
The thickened oil incendiary agent. which are collectively group:"d under the name "napalm" are intended to cau e bum by mean of dlre~l adhesion of the burning agent to the body and by instigating combutlon of clothe • heu e ,vegetation and 0 on. Bumill.g hydrocarbon fue~ are characterized by the production of truck, black moke (carbon particles) co~-
iderable heat and a tendency to produce carbon monoxide un1es there I very goodventiIation. Thu the ca ualty effect of napalm~e due to. a. variety of can es, the ignificance of a particular cau e depending upon the circumtance ofu e, ueh a the quantity fthe incendiary agent u ed, the
amount of 0 ygen available. and 0 on. ... ..
The e factor are iUuskat.ed in a pilot experiment by Montz and hi colleagues (Moritz, Henrique • Dutra & Wei iger, 1947 . They c~n luded that expo ure to burning hyd~ carbon fuel in an encloed pace With good ventilation may lead to death within two minute at 600PC and five to ~x
'. ute at 2S0°C .. Death may be due to. two mechan.i m . Fir t, sy tenuc
mm .~. . .
hyperthermia (heat troke) result ~om the overheating of the ~lood du.nng it circulation through the superficial network of ubcutaneou blood 'lie -
eX . Second re piration i prevented by severe burning of the mouth and pharynx, followed by an ob tructive oedema of the pharyn,_trachea and lung .. Where there i bad ventilation. the hydrocarb n fuel WIll bum more
lowly and may even go out. This re ult in a lower tem~erature than where there isgood ventilation and there i. therefore les . likelihood of death from heatstroke. On the other hand, the bad ventilation increases the danger
from carbon monoxide and other toxic fume . .
According to a US Army Field Manual, theca ualty effect of napalm
are as follows:
Personnel CIi! ualtie re ult from B. number of fla!fle effects. Fir t ofcour e .~ conta t with the burning fuel. Thickened f~el tlC~ .l~and bum hot o~. t.~~ target. It i difficult (0 et.inguish,lhu deterring the individual from accompli ~ng hi combat mi ion. Caualtie are al 0 cau ed by the e t~me heat (I -~ FI 400°F), Inhalati n of Harne, bot vapour. carb n. mon~xlde. and unburned hydrocarbon can al 0 pr duce ca ualties, Persoanel I'll a~IIJbo or othercloe~
pace will uffer due to the withdrawal of oxygen from th air. The hock effect 0 flame on the individual i. great US Army, 1960, pp. 3-4}.
A Swedi h handbook state:
In addi.tion to an increase in the number of burn wound.' warco~ditio~ :a~o reduce an increa e in the proportion of burn .wound ~Jth a. ociat d LIiIJune_. p ft ti ue wound. fractures, etc.) and burns With a pecial aetiolegy. A _an ex
0' . . • d . he t .•.. 11 ery deep wounds cau ed by
ample of the latter can be mennonec tne yp.IC Y vei _
IS]
phospboruaana napalm. These agent a!. (I add the risk of 'y temic poi, oning from white pho.pl'loru and carbon mono ide, respectively (Artur on. 1'966, p, 329; trim. from Swedi h).
More p cifically, the variou ffect of napalm may e ummarized a follow:
] . Heatstrake (hyperthermia). Some evidence . ugge t that immediate death from napalm attack. may be Ie frequent than has otherwi e been . uppoed, since the short duration of the firebail (about 6-110 second )! i_ too short to cause heatstroke. However, the air temperamre cia e to the burning napalm rie to orne 800-I200°C and perons exposed to thi temperature for more than a very few minutes may die rapidly fr m heat. troke.
2. Pulmonary burns. Tho e clo e to (he fire may uffer evere burning of the no e. mouth and pharyn within a bort time a are ult of breathing in the hot air and fume. The phy ical damage to the ti ues, combined with the oedema which thi produce, ob truer respiration and may cau e rapid death.
The dense black sm.okefrom burning napalm and other incomplete products of combustion may causede/ayed pulmonary oedema, even In person not apparenUy burned by the immediate fireball or by direct contact of napalm on the body. A noted above, such pulrn nary complication have come t be recognized a . a major cau e of death in peacetime experience. and very likely contribute at least as much to death' from napalm attack.
3. Carbon mono ide poi oning, Hydrocarbon fuel. uch a n palm, produce carbon monoxide when they burn. Where a victim is confined in a badly ventilated pace containing carbon monoxide the proportion of earboxybaernoglobln :inthe blood may reach a lethal concelltrati.on(66 per cent: ee chapter 4), This circum tance i likely to occur relatively infrequently in the ca e of attack by napalm from the air, but relatively frequently where napalm is projected y flamethrower into clo ed pace
uch a pillbo e . The effect f carbon monoxide and other t ie ubstance are di eu ed further in chapter 4.
4. Oxy en starvation, Burning napalm u up large quantiti of oxy-
gen and in c nfined areas there i po ibility that the level of oxygen may ink below that necessary to upport lite ( ee chapter 4),
5 .. Shock .. Shock due 110 the 10 . of bodyf1uid is a functi n f the e _ tent of [he body urfaee area burned. A cording to Do Xuan Hop (1967), even. when napalm. burn do not exceed W per cent of the b dy surface area of the per on' affected. hock c ndition are neverthele u ual and
eriou . Thi may be due to the fact that hypovolemic hock i c mplicated by neurogenic hock as a re ult ofthe inten e pain r fear, inhalation injurie and the to ic effect of carb n monoxide. benzene and pho phoru .
] 2
Ge tewitz '1968) report that 71.4 per cent of early death arc due to irreversible h ck 0 acute carbon m no ide pining.
6. Bum wound . Napalm is pread in clump of burning jelly, which may burn for up t me 10-15 minute at temperature exceeding OO"C. depending on the cornpo iti n ( ee chapter 2). Beneath the clump of napalm. the temperature i relatively low, unless slag ha been added to increa e the downward heat now. Unle s the victim inadvertently pread the napalm in an attempt to remove orextingui h it, napalm bum are typically round. with an area of inflammation and welling around the bum and a le . damaged area in the middle, According 1:0 Hashimoto 0971) it ha been demon trated that the ti ue beneath the burned area remain above the normal temperature f r five or i minute after the fire i quenched. This cause further Ii ue damage and local thrombo i and necro i pread rapidly in the fir 1 h urand day. the wound becoming ea ily infected.
Becau e of the high burning temperature and e tended burning time of thickened ga oline fuel burn wound reo ulting from them are typically deep and extensive. Ac ording to Do Xuan Hop 1,967) and Ha him to (1971) ome 7 per cent of napalm bum e tend into the .ubcutaneou ti sue and involve mu clesand bone in afurther 1.0-15 per cent The report of Ge tewitz (1.'968) and Hashimoto (1.971, ugge t tbatome twothird of the victim have total area of bum of up to 25 per cent ofthe body
urface area and ne-third have bum' ofm re than 25 per cent,
7. Ph iological complication. The phy iological complication of the burn injury a outlined above page 136-142) al 0 occur in the case of nap tlrn bum. The ch racteri tic weight 10 in the patient. may be a- much as I kg per day. In the Democratic Republi f Viet-Nam burn iniurte have been reported as in urring weigbt 10 e averaging 15 per cent. of normal weight (Gestewitz, 1968). This i due both to evaporation of water from the burned area and mobilization of the body' . fat and protein to compensate for the heat 10 re ulting from the evaporation. Such change are likely t be particularly difficult to cornpen ate for in patient who are initially undern uri hedand an ernie.
The e metab Ii hange are frequently omplicated by injury to the
kidney and liver. ga tric ulcer . decrea e in the blo d protein level ,di - turbances of the hormone balance, psychiatric di turbance • and o c n, a described above. uch development are particularly likely where only limited medical f cilitie are available, a in many of the combat : ituation where napalm weapon have been used.
8. Infection. The area of dead ti lie cau ed by [he bum i. easily infected. Sep i of the wound may e tend the depth of the necrotic ti ue, converting a le eriou burn into a full thickne injury. Due to the general decline in the patient' phy iological and nutritional tatu a a re ult of the burn, infection i parti ularly Liable t devel p rapidly from 10 al ep i (0 generali ed epticaemia, threatening the life of the patient. A n ted
1.53
above exceptional medical re our s are required to prevent and treat bum wound ep i ,re ource which are unlikely to be immediately available in an embauledarea.
It may b concluded that the exten ive tactical. u e of napalm in the Pacific theatre in World War n, in Korea. in Indo-China andel ewhere ha re u;llted iJl a high mortal'ity mong tthe per on affected. Yet there i too lit.tJe. published informalion to enable an accurate asses ment of the m rtality t be made. Some author , have gone 0 far a , to describe napalm as an "all-or-nothing" weapon (Dudley, Knight, McNeur & Rosengarten, 1968).
The eommonoffe.nive agent j napalm (jell'ied petrol'eum) dropped from aircraft. However. Ihi i an ell-or-nothmg weapon and justa it wa not II ual to b called upon to treat bay net wound in World War I Or II (Taylor, 1953) it i rare 10 ee napalm burns: in 3 month we did nol encoumer a silngle in lance, (Dudley. Knight. Me eur & Ro engarten. 1968. p. 334
Other author. uch a Do Xuan Hop (1967) and Ge tewitz 1968). report on the basi of tudies carried out in the Democratic Republk of VietNam that 35 per cent of the per oasaffected died immediately,that is, within 1 to 20 minutes, Unfortunately, neither author give detaiJsa. to the circurm tance under which the victims were affected.)
Tho e who' urvive the initiall infliction of eriou bum are faced with a great variety of potentially fatal compUcatiol1s over a period of week or month. Do Xuan Hop 1967) rep rt that in addition 10 an average of 35 per cent immediate mortality. a further 21.8 per cent of victim die in hop.ital-a total of 56 .. 8 per cent, After an investigation in the Democratic Republic of Viet- am Gestewltz (.1968) reported that 62 percent of affected per on die before th wound heal. Dreyfu (l971)ay; "1 do not have definitive stati tic- but it eem that only about 30 per cent of those wounded by napalm and not killed outright can be aved' (p. 1'9 ).
The minority of vi tim who e live are avedare faced with varying degree f phy i al di ability. characterized by ugly car and contraction . Bum from napalm rno t typically occur on Ul unclothed areas of the b dy, particularl,y the hands, bead and face, and feet and legs. Becaue of the thin layer of ti ue ver the e are , napalm burn rapidly affect the und rlying rnu cle , tendons and bone which greatly complicate the
urgical problem. Recon tractive urgeryto treat lIch condition require a long erie- f operation ver everal years andi unlikely to be availab.le to ordinary p pie in mo t ocietie in wartime condition. Thu • in the Demo ratic Republic of Viet- am,
a limited number of gra el burned person Can be treated in a. general ho pital, e ,pecia.lI,y In e in Hanoi, bU.I: the majority of victim are treated in the v.illage maternity infirmarie and Inc district h pita 1 where skin grafting i not: po ible. I!ns!ead of grafting. wounds are lefl to neal by low kin exten ion from the wound periphery. (Dreyfu , 1971.1'. I)
Ii 4
.... .' . .. a wound which might. heal in two month w~ere
In the e condition • ..... hi. ith iut grafting,
graftingi carried out might tak a .. year. or more. to . ea W.l. thOUb' urn took
,. . . done' ·yea.r after 'e' U . _
A child who e entire : calp wa . an open woun .. '.'..., .
lace wa . ob erved by Con table (pel' onal c.ommu~,cauon? In a . out~
P, h. ital, Do Xuan Hop (1967) reported that With the treat
Vier-Name e 0 p. ., 6'7.1.[ f
ment facilitie available in North Viet-Nam at that time. .. per cen or
. . . h l d within 3 months .19.8 pel' cent. between .3 and 6
wounds 1!'Il survl,vor ., ea.e .. . J. . , 14
month ,and 13.1 per centtook longer than 6 mon~ . to heal. .
Dreyfu 1.971 urn up the ituation f the urvivmg ca ualty of napalm
attack as foU w ; ,
f· - I 'I· eriou after-effect .. Retractile. kin and .col1traCtlO'" of
Poor gra tmg a 0 eave .. <L .. '.. hi
. ... hich will need further treatment. Keloid and hyperu:op !c
ca fo:m .. huge well~ ~. ad inhibit the normal ela licily of the-kin, which In sea will l' rm to urn n ..• . .. . b The e ca are pr ne to turn inhibit the normal movements of the rnern er: ." .. 1 f"1 . d
.. . . and microderrnic inf ctions. The new k.m I .. extr~me y,~gle, n. py dermic. hi d: ki will alway be usceptibl to minor infection that II normal
clero-atrop Ie _ In •
kin would ea ily combat. .. II." th eectre
La fly e ncerning the medical effect of napalm recovery. I. e.re I . e spe f
• ... Old burn cars : how a frequency of kill cancer out 0
of econdary cancers.unc uu , . f pino-
.- .. t such ap' pearance in. normal kin. Thi cancer con I t .0
proporucn to suer ,. .. .. b f the rapid inva Ion by the
cellular epithelioma with a ne allY: pregnesi ecau e 0_
maJignall1 cell of the rel~te.dganghOnar~~1 ... ... ate after long and eo tty treat-
Though orne of the Victim may parua ~ r:cuper .. ~ .... .. (0 _
ment, nothing much can Itl done for the .maJorny ,of napalm-burnedper ons. fey
fu , 1971,. pp, 198-99)
Compared with ingle penetrating w~apon uch a low velocity b.UlIet ' na alm mu t be regarded a an exceptionally cruel we~pon: There I a 0 fr~mentary evidencethat a higher pr~portlOl1 of'casualtie die from ,napalm
bum compared wi.th projectile injuries, that ~hea.dvent of ~eath .1 I~~e prolonged. and that rehabilitation of the urvivor L m.~re d~C~~t.fr ...
i 0 then napalm may al 0 be regarded as more. effective .. om a
, '. - rative : tudy ha ap· peared In the
military point of view. Smce no com pa :. . . .... "' . _ be
public literature any judgement as to whether theexces Ive. cru.elty can
ju tifled by the claim of military nece ity i likely to be ubjective,
White phosphorus burns .,.
White pho ph ru ha been u ed exten ivel.y. a a. moke, Jnc~ndlary ~nd
• . .. I, .. • mall arm arnmunitton, grenades. artltleeysheils,
anti-personnel weap nUl. ... .. _
rockets. bomb, and annper onnel mme
. Id (ll .. .) amongst British troop. during
14 Of 3977 admission due to burns and. 'sc,:t a cau e "monlh61 per cent for
Wor.ld War I, 76. 7 per cent were hoSPI~~~~e~rfO;~;e t~h:n 63 month (Mitchell & Smith, betwe n 3 and 6. monrbs, and 1.97 per ... d b 0 Xuan Hop renee! both the depth of 1931). It eerns .likely that. the flgur . re,po;e .. ~nd °lhe -limited medical facilities available
napalm bum compared with many other Y~. . c ... . ical treatment.
in the Democratic Repllblic of Viet- am, particularly for long-term u.rg . .
15.5
W:hite ph~ phorus bums havecertasn eharaeteristics .. Becau e [he parIHc'les ·of white phosplil.oru . are usually di-b"iibuled by an explosivecharge .. thee particle .rnay penetraee deepl,y into Ute kin. Secondly" the phosphOlrllll may continue to bum. for hours, and inome cases days, until it .i .' neutralized by some means. For thee reasons, phe phorus bum tend to be made up of mall, deep, lesiees.
During World War n there were several report of death from the toxic action of white phosphoru , contained ill tracer bullets fRabinowirch, 1.943; Cope, 1953), which made up 2 per cent of all missile wound (C. G. Rob, in Porriu" 11953,),. Porritt (1953.) reported:
WOllnddllcla incendiary or tracer bullets need special management becau 'elhe phocll~llorus theycontai:n cau e chemical destruction of the tis ues, early and progl'essive ,hock, and 8l ri-'k of fataJ hepatic and renal damage if not removedearly (PorriU, 195J,p. 2.9).
The 30~lb incendiary bombs dropped by the Bri!lish on Germany COIltained white phosph.orus, and Bauer (citediin Bend, 1946) reported that "not only laymen butalo doeton called every burna phosphorus bum". However,. Bauer tales that "no ca e have been reportedin whi.cl1 organic damage nLu~ting from the absorption of pho pheru through tlilekin ,could be proved".
Thirty years ago any tox:icity ofphospheru in bum. woul~d probably not have been observed since' everely burned pauenu usually died. Since World Wa:r II, the treatment of bum bas improved considerably, wilh the re u~t. that. the death ratein the bet modern cendition has decrea ed, With t:his decline in mortality the everity of whit'e' pho phorus bums compared with wound. from other burning ubstances has become apparent frem a number of recent studies, Because ,of it i;mportance the que tion of the toxic~ty of white phosphoru weapon i discu sed in depth in chapter 4, while this ection is restricted to a de cription of'rhe bum wounds re uUing from the e weapon - ..
Many author. di t.illguish between thermal bums, due to heat and flame, and chemical: bum, due to the actionofa chemical! . ub ranee on the skin. Thi . terminnlogy is ambiguous, since the production of heat and name is the result of a chemica] reaction. Nevertheles , for dlll.J.ca:.l purposes it i useful to make the distwnction since, in general, flames must be extinguished by the exclusion ·of oxygen, whereas chemical ubstances must be neutralized or diluted.
In the case of whitie phosphoru burns initial injury Is largely "thermal" rather than "chemical", but elemental. pho phoru ., or phesphoru cornpound produced lin the wound, may be re ponslble fur ubseqsent compl:icatioli1. For IhL rea 'on, most. author cla ify white pho phoru bums as ~hemical rather than purely thermal (for example, Curreri, Ach & PrUItt, 1970).
156
The I'.rin.cipa~ difference between thermal and chemical burns, including white pho .photllls. bum, i . the lengl.h .' f time during which ti ue destruetien continues, since the ,chemical agenreemlnue to' cause damage untii Inactivared by reaction with the tissue. neutraliaing agents .or dilution with water (Curreri, A ch &, Prui.tt, )'97.0),. White phosphorus tend to bum h_ w.ay through the skin and, even days after the original, injury ,.pont.aneu ly igniting particles may be found deep in the wound (Jane, Peter' & Ga ior, l'968).T:hail: is, white phosphorus buens are uually ef' second all' third degree, The e bum ar,e rna II: frequently localized 011 the arm, hand. thigh, lower leg and head. Becau e phosphoru i lipidsoleble it ·pread.rnpidly through the fatty tissue underlying the dermi (Summerlin, Walder & Moncrief. ~967) and. the phespharus-derivedacids produced In the wound may cause further tissue damage (Rabinowitch, 1943)1,
The most frequent. complication are contracture of the joints with resultant functional IossvInjuries jn the head lead toa significantly high incidenee of eye complication_ .. Other cemplication such as wnflamma.tion of the cartilage' of the ear , gallgrene of the finger and pneumonia can be ob erved in 1.0 per cent or more of the patient (Curreri.et'al ... 1970).
The estirnati ,n of bum depth by cllin.i.cal observation following chemical injury i difi:icult.. The evere fun thickness chemical burn may appear de,cJep,tilvd.y superficial with onl.y a greyish-brown discolouraUon of intact kin during the first few days. (Currer] et at. 1970).
Surv,eying the surgical Literature re ullin!! from World W.ar U, Cope fl,9S3), reported cases of wounds caused by explosive bullet which depo ~t,ed phosphollU . in deeper tissue . Hea[ing ef'these wound was lower than normall (Cope, 1953, p, 308).
DurililgWorl.d w.a.r n phcsphcru was u ed in bombsa wda ill bultets andheU. Cope (1953,), records the ca e of two children injured while playing with an unexploded phosphorus bomb:
The two children. aged 7 and 8 wer accidentally burned whil~epliilying with a pho phorll bomb on Sully 27, 1943 .... Cbilld A had exten ive second degree. bum on the backs ofthe legs. an.d thighs and a: patch offull thickness destruction onthe back of the left thigh about 4 in. quare .. Ch:ild B Wi! more severe~l!y burned and bad J'ost the kin from thegreaten pari. of the back of the rigllt leg from the gluteal region to the a.nkl'e and 0111 the left side fliorn the glutealregien of the knee. She a.l80' had spla sh bum on the face and right hand ~lnd arm , .. Tbern.(,e ?f healing was sl~ow in both case and multiple grafting operations were done blllt lit wa mn until, December ,of the same year lhalepit'llelialisation was, complete, The scars which are e from the e bUl1ls were in both ca e keloidal and un table, AClive contraction took placeneces i:tating re-excjsion and Thierrch grafting inane case and X··ray therapy in the other (Rook-down Hause Centre He pi.taJ aceount, cited in CO,pe, 1953, p ... ]10).
The longer time required to. heal. pho phorus bums wa reported by Obermer (~1943) and Sinilo 09M). _ his has been recently confirmed by Currie'; et al. 0970), who,analy ed llleases of whi:te plilosphoru iand other
[57
chemical bum patient admitted to the U _ Army In titute of Surgical Re earch during the period fr m 1950 to 1968.
The mean total body urface area of the burn wa 19.5 per cent as compared with 28.5 per cent for all bum patient, admitted during the arne period, although the mean area of third degree (fuUthickne ) bum was 10.5 per cent f< r aoth group. The lower total bum area in the chemical bum was reflectedin a 1 wer mortality: A per cent compared w.ithI9.3 percent for the non-chemic I bum adrni in. However, Inger ho pitalizalion wa required for complete kin healing of the chemical burn than for the overall group: an average of 104 h pital day compared with 74. or an Increa e of 40. per cent.
An average of 5. .. 8 urgical eperaricnsper patient wa required. 78 per cent involving homo- or autografting of third degree burn site . Table 3.10 how the 22.7 complication that were recognized in the I. II patient, the most frequent being c ntractur .. of j inc (52 ca e ). and c mplication f the eye and eyelid (36 case ). Table 3.11 how the di tribution of the contracture ' which re ulted,
Systemic complication uch a pneumonia lO ca e ). upper gastrointe tinal bleeding ( ev n ea e }.. epticaernia (five ca e I, acute renal failure (four ca e), jaundice (three case and urinary tra t infection (three c e) further complicated treatment. y temic complication re ulting from ph phoru burns may be due t hypovolemic h k, or to the toxic effect of phophoru ab orbed in the body fluid through the bum wound to toxic effect of sub tances, uch a copper sul!phate, IJ ed to treat the wound, or to
combinati n of the e fact r .
White pho phoru bum from e ploding munition are often a ociated with other injuries such a laceration .fragment wound. traumatic amputation of one or more digit. and fracture of the long bone. Table 3.12
how the distribution of uch as ia~ed injurie in the US Army. tudy.
In me ca e p rticle of pho phoru may penetrate deep into oft Ii ue or into the che t or abdominal. cavities. There i u.uaUy a need for radical debridement beeau e of the depth of th penetration nd it i extremely difficuh to remove all the p rticle .. US Army recommendation. in Viet- am
tate that re-debridernent hoald be planned after 6-24 hour ,by hich time the continued burning of previou ly undetected p rti le will have created more clearly circum crib d area . of burned ti . ae, enabling the particl to be I cated more readily (Whelan. Burkhalter & Gomez. 19 ).
There L n doubt that bum due to white pho phoru . weapon are etremely eriou . Not only d they hare the characteri tic of thermal bum but the wound take longer t heal. By continuing to bum in the w undo pho phoru present eriou problems of treatment and re ull in deep wand which may require e ten i e urgical e ci i n. In ddition. the known toxicity of white pho phorus i a hazard which may re ult in complication uch a kidney and liver damage. alth ugh publi hed
158
Table 3.10. ClassirlClltlon or 227 compLications rollowing white phopborus and otber e:bemleal bums In .... total of HI patients"
Per cent
Contractu re fjoi n LsD Ectropion
Chond rill of ears Gangrene. one or more ringe C taract
Pneum nia
A:nkylo i " one or m re interphalangeal joints
Upper gastr inte tinal
bleeding Corneal ulcer
Celllliiti or Iymphangili Cutaneou ab ee Septicaemia
Acute renal failure Infected fragmenl wounds Osteomyelitis
Jaundice
Urinary tract infection Other _
Totall
52· 18 1.7 [7 II 1.0
7
7 7 6 6 5 4 4 J J J
47
2:27
22.9· 7.9 7.5 70S 4.·
4.4
3.0 3.0 3.0 2.6 2.6 2.2 1.8 1.8 1.1 1.3 t.s
10.7
Joo.O'
II See [able 2.11. below.
SOUT e: Curreri. A ch & Pruitt (1970).
Table 3.n. Contractul'es resulting in fUIICti.onal d' bUlty asa result of white phosphorus and olher chemleal burns"
L cation
Hand II
Finger .10
eck 9
Elbow 7
Axilla 5
Wrist 3
Mouth 3
nkJe 2
Knee I
Perineum I
Totllil 52 d See foot.n te a. table 3.10 for explanation. SQUTce: urreri, sch & Pruitt (1970).
159
Table :J.U. Mechaniad iqjlll'iesassociated wltb while phosphorus and other chemt-
cal burns in a lotal of lllpatients" - -
ype of i'1.iury
umber of injurie
MUltiple leceratlons or
uperficla] fragment wound 17
A mpu [ tion of one or m re fi nger II
racture, open 7
, racture, clo ed
Major nerve orartery injury
Penetrating wound of the cornea 4
Penetrating wound ofthe abdomen J
Perforation, of tympanic membrane
(unilateral! or bilateral) 3
Penetrating wou nd of the chest :2
Los ofteeth 2
Total .. 59
9 See footnote .a. table 3.10 for explanation.
Source: urreri, ch & Pruitt 11970).
research do n ,t indicate clearlythe e tent to which thi hazard L a major factor In battlefield ca ualtie . The question i further examined in chapter 4.
Thermal radiaUon bur:nrrolll nuclear weapons
No a. count f therm I effect of rn dern weapons would be complete without reference to the thermaJ effect of nuclear weapon.
Depending upon the nature f the weapon, the fraction of the nuclear e'xplo ion yield erniteedas thermal energy range from 30 to 40 per cent at. an altitude below 30000 metre .. The di tribution of nergy may be r ughly e timated a in table 3.13. Thisthermal radiation i emitted as a pul e of extremely high energy of hcrt duration. For a l-kUolonlli air burst. the effective durauon of the thermal pul e is 0,3. econd . For a 10-megaton air burst. it may be a long a 30 second. Roughly peaking, a uming appr ximately n -third of the energy i emitted a thermal. radiation, it may be estimated that for every kiloton exploded orne 3.3 X Wil calorie. are relea ed in the form. f thermal radiation (US Department f Defense, 1962).
It has been e tirnated that on the ground immediately beJow the Hiro-
hima bomb e pi ion. which had an effect ofome 1'2.5 kil'oton and took place at a height of.560 metre, ,lid material were heatedteabout 3.000- 4000"C and at I 200 metre away temperatures exceeded I 600"C. However the thermal pulse from a nuclear explo ion j 0 hort that while
orne porous materials . uch as lightweight fabric, paper and dry gras may ignite, wo d may onl.y cha:r but not ignite. Surface temperature are
1$ A Idloton i the nuclear equivalent of 1000 Ion of TNT high explo ive; a megaton is the equivalent of ene mUH nton of T T.
160
Tab.le 3,,13. Dlstr:lbution of total e.Dergy ~eJeased, ~y a typical nuellal' explosion In
air at Bnaltirude below 30 000 metres .
ource
Per cent energy
Shock and bIa I
Thermal radial ion
Initial ionizing radiation Re idual'ionizing radiauon
50 35 j
10
Duree: US Department of Defense (1962).
highly dependent on the reflective propertie of the material: light coloured material refle ts the heat rather than ab orbing it. whereas dark material ab orb the heat
Nuclear explosion rnaycau e burns both directly and indirectly:
One of the mo teriou consequence of the thermal radiation from a nuclear expl i n is the production of "fla h bum" re ulting from the ab rpti n of radiant energy by the skin of e po ed individual .In addition. becau e of the focu sing ction of the len of theeye, thermal radiation can cau e permanent damage to the eye of person who happen to be looking directly at the ur tift (US Department of Defense, 1962, p .. .328),.
Iti e umated that 20-30 per cent of the fatal ca uaIties in Hir hima and Naga aki were cau ed by flash bums.
In pite of the thou and f case experienced in the Japane e explo ions only the general feature offla h bum have been de cribed. The e observaLion have since been upplemented with experimental tudies u ing the kin of pigs which ha many imilar characteristics to human skin (Pearse, Payne & Hogg. 1949). In addition to being largely limited to exposed area ofthe b dy .fla h bum. generally how a mallet depth of penetration than do flame burn becau e of the hort exposure time Ie s than one econd in the Japanese explo ion). everity of 11a sh bum in Japan ranged from mild erythema (reddening) to charring of the outermn t layer of ~hekin .. Healing of bums in. survivors wa hampered by inadequate care, poor
anitation and general lack of proper facilitie re ulting from the general widespread de truction,
in addition to the primary effects of thermal radiation, nuclear weapon may ignite tires in two way. Fir t, thermal radiation may ignite combu tible materials, typically paper. rubbi h curtain and dried gras • Which in tum ignite more olid fuels such at wood. pia tic and bitumen. Se ond the blast wave can up et stoves and furnace I cau e electrical hort-circuits and break gas mains. The outbreak of uch secondary fire is djffi-
II A recent report of a group of expert convened by the International Commlue or the Red Cro point to the fact that La er weapons, which are at ,pre enl beiog developed (Meyer-Arend I, 1968), may have imilar effeCI on the eye (leRC. '19730). An experimental
tudy of'flash-blindne r i desernbedby Chisum (1968).
12-743168
161
Table 3.14. Comparative mortality doe (0 beat, blast and ionizing radiation Jn first· da univorsln :Hiro hlma
Total
41992 45356 37 657 125005
33.6 36.3 10 .. 1 100 .. 0
9TI6 475 :5 649 18 900
51.7 18.4 29.9 100.0 umber of urvivors on first day
Per cent of total number of fir. ,-day survivors Number of deaths 00 ubsequent day
Per cent of al.ldemhs
Source: Oughter on & Warren (1956).
cult to predict inee it i dependent. on the density of ignition point humidity, wind and other prevailing condition' .
The ec ndary incendiary effect from a, nuclear attack do n t differ signiflcantly from tho e due t a mas ive u e of conventional incendiary and hi.gh explosive bombs;"
The incendiary effect ora nucle r explosion do 01 present any e peci lIy characteri tlc feature. In principle the ame overall re ult a regard de truction by fire and blast might be achieved by the use of conventional incendiary and highexplo ive bombs. It ha been e timaied, for example, that the fire damage to building and other structure uffered at Hiro hima ould have been produ. ed by a,bQut 1000 tons ef incendiary bomb di tribl.l.l.,ed over the city. It can be een, however. that ince this damage wa cau ed by a ingle nuclear bomb of nly_O kilotons energy yield. nuclear weapon are capable ofcausing trernendou - destruction by fire. as well a by blat U Department of Defen e, 1%2, p. 345).
According to Oughter on and Warren (1956), 45000 people (lied on the fir t day at Hiro hima while 22000 died at Nagasaki:
Bums and blat effect were re pan ible for rna t of th effect on the fir I. day. but since the effects were interrelated, it i impo ible to kno \ hat proportion of deaU) was due to each or them. However. all ob erver are agreed that heat WEI the major cau e of death on the first day (Oughterson & Warren, 1956, p. 95).
According to the U Department of Defen e (1962) about two-third f the casualtie at Him hilf!1a and Naga aki v ho died dunog the firt 24 hour
uffered fr m bum the effect of which were often augmented by other ulJurie and there were many death from bum during the fir t week. [t i e tirnated that roughly 50 per cent of all death were due to bums of one kind or another. Among the survivor after the fir t day, 6 per cent suffered from bum , 95 per cent of which were fla h burn _. The rea on for the low proportion of flame burn among the urvivor i that. "mot
17 It is elimatedlh.at83000 people died in the incendiaryraid on Tokyo. However, rather little has been publi hed on the effect of the incendiary raids on Japan, in contra I to the wealth of material on the atomic bomb attack .
J62
of those who uffered flame bum did not urvive, ince they were caught in burning buildings and could nate cap "(U Department of Defefl e,
J962, p. 56 ).
In Hirohima alone nearly 42000 fairly· eriou burnca es were reported
among the survivor of the first day. Of th e, 23.3 per cent died ubequently, compared with 7.7 per cent of the 45000 bla t wounded. urvivors and 15.0 per cent f the 38 000 ionizing radiation-affected urvivor
(table 3.14). ..' '.' . . _
Thus there i good rea on t regard the Hiro hima and Naga aki bomb
as largely. and perhap even primarily. in endlary weapons, and only econdarHy a blat and radiation . eapon . Further. the exceptionalJy large casualty tali tic which re ulted indicate that incendiary weapon. may 'be the cause of more erious injurie than either blat r radiation weapon. Thi conclu ion i largely borne out by tudie made f the ca ualty effect of the. trategic bombing f German citie • de cribed in the ne t ecti n,
Mass casualties (rom incendia.ry attack
The air attack on German citie during World War HIed t the death of between 500000 and 800000 people." Several rep rt were prepared on the cau e of death in the raid. during which the Briti h Royal Air Force dr pped 196335 ton .. of incendiary bomb and 2~4 312 ton of high explosive bomb Harris, 1947) and the U Army Air Force a further 80000 1.0," of bomb ,(US Strategic Bombing Survey, 1945) on German populati n centre -a t tal of 510747 tons, or appr irnately one ton for
every fatality. . .
The Medical Branch of the Morale Divi ion of the UStrategic Born 109
Survey publi shed a, report in December 1.945 on Tile Effe . .t of Bombiflgon Heal/hand Medical Care ill GertllQIl which included a chapter n the nature of air raid c ualtie by aptain Franz K. Bauer. Bauer concluded in part:
... It can be t, ted that there is a definite relation hip between the type of mb
dr pped, and the ty,pe of death r injury 10 be e peered. An incendiary raid expected to cau e more dead than ounded, through the ,effe~t . o~ heal and carbon mono ide: in bombings\ith high explosive . mechani al injun ' outnumbered
death", .
. . . In allthe cities visited carbon mono ide poi oning w •. regarded a' the pnrnar
eau e of death or injury." sometime' reaching 10 a much,a. 80: per cent of ~II incendiary raid ca millie'. ir blast wa found to be a relative I mfrequenl ca~ e of death and affected only people within a radiu of 30 meters from 11'11: explo Ion of a bomb (Bauer. cited in Bond, 1946. p. 113).
Bauer' report ontain considerable interesting detail. It became - pparent to leading German pat hoi gist that the ir war wa leading to
Iii ee ch, pter L
163
1:Bble, 3 •. U;:. Most prominent causes of deatb as a ,r un. ,of 'tbe w.c,endillI',Y fllid's on Uamburg.luil.~ IUld August 1'943
Causes ,or d'ealh froml aterna:l iinj:ury
I .. Burial under rubble and debris, and injllr:Y lir1)m flying frogmen I
2 .. Sec:onclaryi,njuries through explo ions (drowning, scalding" chemical bums, poi aning from
the by-pruducts oh:~ploded bomb) -
3. BUrns
4 ... Tetanussecondary to bums where no serum was given prophylactically
Cause_ ,of,deajll 'liroml lntemallnJury
I. ,. arbon monoxide' poi ening in airrnidhellen and occurring during rescue work
2. Effect of.heal InroughcollduC:lion .and ~d~allionin, the presence of very higb temperatures
3. Over~ealmg over a prol~ngedl perIod of lime Ihr,QlIgh temperatures Which,. norIllllJly,can be telerated :for hort :penod ,only
4. DUSI inhalation: blocking of the upper re piratory passage and ini1alal.,ion, w,ilh damage
f the mall bronchi and aJveou
5. Carbon ill1onoxid'epoi oning 'From bur 'ling ga mains
6.udden heart death rhrough [rigfU and exnau ·tion in cardiac patient
7. BiaSI i.rU~ri~s in which eXI.emal injuries may be' a.'bsent or which may be ma ked, by ex-
ternal mJLmc . .
SOl/Nee: Conclusions of a meel'ing of expert ealled 'by Iheinspector of anitary and medical matter .f the LutlwalJ.e held in J1U'1 rborg, December 1943; reported by Captain Franz K. Bauer: US . rmy _ Medll::..al Corp. '''The nature of air raidea uahies", 'in US Strategic Bom'blng . urvey, Morale Division, Medical,Bl1Inch. Th« £jJe,'" of Bombinl!· Oil Health and
Medkul Cure ill' German), December :I,945;cil.ed by Bond 0946}. -
c-auses of death which were not at first obvious, In 1943 measures were taken to en ure correct diagno e . AU per ons with unclear diagnose were sublecred ro autopy: between 20000 and .30000 autopsies were carried out during the war.Phy _ichms from die Luftwaffe were appointed to supervise commissioas whose task was to study the caus es of death, Prior to the e tablishmentof the e cornrnissicns a meeting of ,experts was called in JOt'erborg in December 1943 to discuss the effects of the raids on Hamburg in July and AUgln 1'943. Tbeir conclusion as to the most pr'omiinent CB.U e ,f death al tha.t time are shown in table .3.16. Several theorie rega:rding death from anoxia, "carbon dioxide poioni,ng", "gas poisoning' (that is, • 'pho phoru _ gas") or frem highfrequen.c.y wa.ves . ubsequent to explosi.olls were disproven.
Additional studies after 1'94.3 led to more understanding .of thecauses of death, In addition. to mechanicalinjuries onllY beat andcarbon monoxide pmved to be of stati tical importance, In large-scalefires, deathsresulting ["om heal and carbon monoxi:de paion:ing outnumberedthose from mechani. cal cau es.
The effect , of heat were .of two kind in large-scale incendiaryanacksuch a those on Hamburg:
0) The ,effect of direct heal of hort duration through conduction or radiation with production of bums pro per.
(2.) The effect of hiigh t'cmperalure over long period f time which did not limmediately lead [0 protein coagulation. bUI which caused a syndrome identical 1.0 that of heatssroke. (Bauer, cited by Bend, 1946, p. 115)
I! 64
Heat troke depend ana number offactorsuch as the, humidi.t.y of the air .. the ces arion of weat production and the amoullt of heat ~o' which 'he body has been ,expo ed, In humid air heatstroke may occur at a. temperamr,e of60~ and. i . not necesaarilyassociated with subject.ive 'complaints.
his accounts for rile many bodies which were round dead in room from which e cape would have been :1'0 silble. and which were ina po.sitiolll not suggestive of agony before death occurred (Bauer, cited by Bond. 1946. p. 115).
According to Bauer, police engineer in Hamburgestlimatedtbat temperalures in the burning city block irose as high as 800DC.
Literally hundred of people were eel! leavj,ng heltersafter fhe heat became illl'en e. They ran across the street. and were, • een to collapse very. lowly like people who were thoroug:hly exhau ted. They could no! get up (Dr. Helmuth B:miecki 'of Hamburg)" ..
Mot of thee pe pie were not 'burnt to ashes when: recovered, but dry and sbJ'iun'ken. resembling mummies. In many the intense heat had cSiu_ed the skin to, burst and retract over typical area- uchas [he ,elbow. the knee. the calpand the orbit Baniecki thoughtt:hat the can e ,of death in these cases wa - hock, hl .approxi.ma(ely 80 autopsi - . he found all ,orga:ns shrunken, howing venous sta L withim::.rreased permeability ,of Ute small blood ve sels .....
Profe sor Rose" chief consultant [0 the A:ir Ministry,. ummari~ed UiI.!! effeet of heal .. Be ide immediate contact wirh names, he wrote. the effect of heat through hot air a well a .. radiation of hot gase and from objects is imponant, T:lili aceeunts for the evere heatchanges ill women who do not wear more than tock::iings on their leg • or not ,even tocking. In many cases, when : tacking were worn, they were :not even singed. .aItboughthe skin ancIunderlying . tl1Jclu,r'es. were
everely damaged. Radiation heat of over 22 OC can il1Uame, clothe and [hair J.
Beside thi 10ca.1 effect of heat, o,verrburdeni:ng of the hea.l-IFegula.ting mechanisms of the body is important .....
During e cape from overhestedshelter tillfoug:1l bll.ming dty bl ck , the danger was chiefly from radiated heal. The inhalation 'Of hetair can can e : evere d mage to the re,_pirelmy passage, such as 1!J'lcerou necroses of tile muceus membranes. Wbether thi isa separate entity or the changes apart of the wbol.e piclUre which leads to death i a: yet un olved. It _hould be kept in mind that the inhalation ofdangerou ga e or by-product .01" fire mill ~. beconsid:eried .....
Thedegree of temperatures produced ill incendiary raId gave rise to a. ,tlJ]c-ti.on from the office 0:1' Profes or Karl Brandt,commi sarfor anita!"y and heslrh matter for Germa,ny .. Pro~e or Shuetz, a phyiologist. of Muenster, answered fmmthe Iasnture of AviistIon Medicine: The questionconcelCl1edi the effect all. the human body 'of overheating to. 410C for eight hours, The answer is: inlhe tissues increased temperature up to 50·' is followed by death 'of all cells. wirh . ub-
equent vacuolizatien: higher lemperatureareFollowed by shril1:k:i,ngand falling apart of the cells, According to Ludwig Asc:hofr, human cells die 31 50·C. ve ides form .in the Ii sues at 51,~C, and haemoly-i- occurs at 60~ . Gangl.ionic eel] . are de troyed at 43° . Animal die exposed to temperature , of from 6{l°C to U)OOC ill overheated rooms, u uaJlyin cenvul ion, after II few minut,e 10 .balfllDl hour (Bauer, in Bond. 1,946, p ... U6),.
Bauer give' the foHowillg de criptlon of the victims of the Hamburg attack on 27-_8 July m943, taken from anaceount of Prete or Graeff,
16.5
consulting p.EUhol.og"i~t to, the Wehrkr:eis .x (military defence area) ilil Hamburg:
Many of'the bodies were lying, in the street half~cl()thed or nude. The only coveting that they a.lway , had on was their hoes, The victim' hair wa often bumed, but preserved, A few hour" after the start ofl.hern.id the corp e ,had a peculiar a peel; they seemed blown up .. I:ying ontheir tornach . The buttocks were enlarged and the male ex organ', were swollen to the ize of a, child' head .. Oeca ionally [he kin W,8_, broken and indurated in many place, and in the majority of case wa a waxen colour. The ~face wa pale. Thipiclure lasted ollly a tiew hours: after thi time the belie hrank. to - mall objects. wilhahard brownih black s'kin and charring of diUerent part and frequentl,y to ashe and complete di -appear.ance ....
bl the shelter bndlesas limed various aspects cnrresponding to tile C:.ircumstances under which death had et in. Nowhere were bodies feund naked or without dothing as tiley were in the treets."] he clothe. however. of len showed burned 01.11 hole_ which expo edthe kin, Bodie were frequently found Iy.ing lna thick, grea.y black mass, which was without aJ dOUDI melted fat tille. The fat coagulat,ed onthefloor a the temperature decrea ed. The head hair a a rule wa unchanged or only slightly si,nged. The bodies were not bloated except for a few which were' FOllnd floating inwater which had seeped into the helter from broken main. All wereshrunken othat the clothe appeared to be too large. Those bodies were B'ombellbrandschrum.pj1eiclle'l' C'incendi:ary-bomb-' hrunken bodies"), These were not a:!w,ay in one piece. Sleeve, and trouser legs were frequenUy burned off ami whhthem the Iimb were burned to the bone. Frequently such bodies burned to' a crisp week. after dea.th-apparently after o.xygen had: become available .. In the same rooms w.ilh •. ueh bodie Were :~ound other more or les preserved orshrunken corpsesand ah 0 some which had fallen to ashe and couldhardly be recognised. Many ba ernents containedonly bits of ashe and in these cases the number of caslilallie .couldoh.ly be esl'imatoo (Ba:u,er, in Bond. 194,6,p. 1(9).
While Bauer makes no reference liO death loy asphyxiation due Wo the withdrawal o,foxygenfrom the air. many urvivor tated that the air "jut didn't come anymore" and breathing became very difficult. In. the shelter level of ,oxyge,n fell so low that matches or candles wouldnot II)Orl1. and peopl~e lay on the floor where, beeau eofa higher concentration of oxygen. breathing wa easier. Outside, in the city streets, the, firesterrn drew in a mas. of fresh ak with sufficient foree to blow people to the ground.
Accordi.ng to Bauer, carbon mnnoxideas a rnaiorcause of death wa aposs~bility which few had expected before the war, However. carbon monoxide deathsassumed . uch proportion, that the high command of the Luftwafte issued an order to examilliing cornmissicnstcprocure tatistical evidence ·of carbon monoxide poisoning .. The question of carbon monoxide poi Oiling is examined in chapter 4 ..
lV,. lite medical treatment of war burns
In thi c sectionan outline of ome of the problems of the medical treatment of victim of burns ispresented, Such information i necessary for anadequate under tanding of the hnmanitarianissues invol'ved In the use of fire
]66
a. a weapon of war, since pro peets forcasualties cau ed by incendiary weapons are panicldarly dependent upon the quaJlity of the medical treatment available to servtvors.
The treatment procedure .. outlined below explain what can be done for the victim of burns with the bet fadlities currently known to medical
clence, Even with such facilities, thetreanaent of the severely burned is long, tedious and eXceptionally painful-a severe emotional burden on the patient and hi '. family, and indeed, in many cases, 0111 the medical staffas wdL The complexity of a evere bum wound is such that exceptional medical resources are re;qulred to give the patient. a reasonable chance of recovering a suffide.nt degree of functional ability to be able to perferm normally in society .. Even where an adequate fU_1lcdonai result is obtained, scars and disfigurement often presem a psychological and social barrier to normal sodal tit:e ..
The nature of many recent conflicts ha meant that the medical equipment and expertiseavailable to (he confiicHns :paritie: has been highly variable. Many of the facilities required to treat evere burn are, not available or are destroyed in combat. SUch conditions are tantamount to increasing the ,. effectiveness' 'of the weapons. employed, since a greaterproportion of the victims will di:e or be permanently disabled. To thisead, efforts ma:-y be made to reduc-e the medical supportavaila.ble:toan adversary, Suffer.ing will thereby beconsidera:bly in.CJiieased. Due to inadequate trearrnent by skin graft"ing andassociated surgical measures •. a. t.hird degree bum wound may never he-all and the patient wiWID ha.ve to bear a permanendy open wound asa continual urce of hllfecti.on, subsequently l.iabl.e to become cancerous, By contrast, a wound caused by a.low~vel,ocity buJiet orftagment may in general be treated by r,e[aUvelly simple means and the prognosis for the patieacis not 80 vit.aUy dependent upon the ,qlllality ,of medica! treatmentavanable,except. when hi major organs are damaged,
Because of wide variations in. the facili.tie . availabla no preci e coarse of treatment can be described. The fullowing outline refers to the best treatment pos ibl.e but it should be borne in miind that uell facmti.e . are nes available to a bighproportion of the victims ofincendiary attack.
Firs •. aid
It may be a umedthatsome ~I:)fm of 6r _ laid is available tothe majority of war wounded. although :it may be the onl.y treatment a.vaUable. The major point. to note Infir 1 aid an as follows:
L Where possible. flames should be "suffocated" by excluding air. ~o:r example, by covering them witha thickcl.otlil. Where napalm is burning un the skin. greatcare should be t:aken to exclude the ,air by covering it without spreadiogthe nickyjeUy ... Once thetlame_areextinglJis·hed.,imple nap~dm will not ignite puetaneously, However,it may contain white phophoru . in order to reignit,ei't in alir. or sodium loignile it in waterv Phosphorua
W67
fragment h uld be bathed in water r covered with a wet cloth until
they can be removed,
2. To pr teet the ore fr m infection and further trauma, it hould preferably be covered with large, rente ab orbent dre ings or, failing that thepatient may be wrapp d entirely in a heet, blanket or coat. It i important to keep the patient warm,
3. Particularly if he is unconscious. the patient may have breathing difficulties. The re piratory channel may be blocked by blood. aliva, vomit . r the tongue. n is easie t to open the air pas age, with the patient lying 'n hi ide with the neck bent backward' . If the patient doe not. breathe spontaneou ly, artificial re piration by the "mouth-to-mouth' method or. if available, the administration of 0 tygen, may be called f r.
4. In the event. of great pain, which may contribute to neur genic hock, analgesics such as morphlnemay be lowl;¥ (over a period of one to [,WO minutes) i:nject:ed intravenou Iy for adult .. Codein may be given to children for the same purpo e.
Hospital treatment of burns
The hopital treatment of burn wounds i a specialized field ofconsiderable complexity, enabling a certain variati n in treatment method (e.g, Liljedahl, 1967~ Phillip & Con table, undated; Pruitt & Curreri, 1971; NATO 195 ). A brief outline of ba ic therapeutic mea ure i given to indicate theextent of the requirement for the adequate treatment of bum wound
The initiali therapeutic objectives are: a) the prevention of _ hock
(b) the maintenance of adequate 0 ygen upply in the event ofre pirat ry complication, and
(c) the prevention of infection.
Sub equently attention may be given to the surgical treatment of the wound, to psychiatric care and finally to rehabilitation.
The prevention and treatment of shock
The flr t two to three day after the int1ict.ion of the bum injury normally bringfluidl . and oedema. leading to hypovolemic hock which i. brought on by too little fluid in the body, Repl cement rub tituti n of 10 t fluid i the obvious treatment.
he admini tration of fluid volume in hock hould have a it goal: (I) an adequate blood volume based 011 the central venouspressare mea urements: and, (2) a normal red cell mass. adequate protein and colloid. the replacement of defiiencie in extra ellular fluid. the correction of electrolyte and pH abnormalitie in the bl d and upply of ealori requirement'. 0. one fluid i adequat • bUI a
mbination f different fluid .Iailor-made to. keep a normal bl od c mpo ition, is needed. Protein and other colloid are e ential to maintain water in the blo d and. prevent edema. Whole blood eoHoic! and electrclyte are all needed in proper am unt and prop rtion, (Harda ay. 1969. p. 653)
]68
Table 3.16. Typical. replacement ftu1ds for a severely bumed adult during ClIe first l4-1I01lf period
0.5-1.5 ml x kg body weight X per cent body burned 0.5-1.5 ml xkg b dy weight per cent body burned
I 000-2 000 ml
ElecnolYI:I~ (e.,g. Ringer', laetete) olution
Metabolic requirement (5 pet cent ugar 01 ution)
ATO (1958).
It i. u ual to admini ter fluids intravenou ly where bum exceed 10 per cent of a child b dy urface area or 1 per cent of an adult' . The e fluid have three main component. compen ate for the fluid I t from the wound replacement fluid mu t contain electrolyte, e pecially odium ion ,and plasma or a colloidal solution made up of pl!a rna protein 011' a plasmaub mute such a dextran." The mostpreferred electrolyte olution i Ringer' lactate 20 a lution of electrolyte re ernbling the electrolyle compo ition of the blo d. Finally, becau e f the difficuJtie of administering food by mouth in _ufficient quantitie due to the danger of the food getting into the lung and cau ing seriou . complic.ations) .. olutioasot
ugar (for example, dextrose) and fat ernul ion 21 mu t be administered intraven u ly,
Typical replacement fluids for an adult during the rift 24-hour period are shown intable .3.16. The e proportion are calculated on the basis of body weight in kilogrsmrne .. Becau e the ratio of body urface area to body weight i different in children Phillip & Con table undated) recommend a formula ba ed on the area of the dy urface of the child. For each
quare metre of the body urface area of the child, whether burned or unburned, they ugge t '90 ml pia rna and 10 rnl saline per percentage of the burn,22 In addition 1500 ml water (by mouth) or 1.500 m1 ofa 5 percent concentration of dextro e (intravenou ly hould be given for each quare metre of the body urface area whether burned or not.
In general an adult require about 150 ml of electrolyte andc lIoid olu-
I' Dextran J a water- oluble, high m lecular weight (. verage 75000) gluco e polymer produced by the action of Leuconosto mesenteroides on sucro e. It i u ed it a 6 per cent soluti n in diurn chloride in the treatment or hock.
'-0 Ringer' lactate elution i made up r 5.7-6. per cent odium. chloride, 2.9--' .3 .per cent .0dium,laclate .. 0.27-033 per cern pota ium chloride and 0.18-0.22 per cent calcium
chloride. .. .. ,. .
tl Fal ernul ion were introduced by Wrellind ( ehubert &. WrellJnd. 1,961; Wr,clhnd. 1962).
recent composition tried ucccs -fully b the U Army Bro ke Medical en!crcontain
oybean il. egg yolk, pho phalide an~ glycerol. <llI.d .provide ne.C<!lorie/ml. Single OO.ml units of the 10 per cent oy can ernulsi n ere adrnini tered 10 pauenrs over a 4·hour period
through H forearm vein (Wilmor . Moylan &. Pruitt .. (972). , . _.
n For example. a nitle-year-old ,chi,ld, with a, bod.y urface area of 1.11 m~an.d a 30 :pllf cent burn. would receive 1..0 30>:90=2700 ml pia ma and 1.0>(30)( 10=300 mlsaline .n, the lirsl 2.4 hours.
169
tion per percel1!tage of ttl .bum .. Phillip & Con table (undated) recommend a ratio of five parts ce lloid toone part electrolyte but the ratio depend upon tbe individual need of the patient the rneth d of treatment and the .8v,ailabiJity of pia rna or pla rna ub ititutes. Due to h rtages of pia rna in the United State a a result of the war in Viet-Nam, many patient have had to be treated entirely with electrolyte elution (Ringer' lactate). Where eleetrolyte solution alone i u ed, n formula can be given and the amount is determined by urinary output and ven u pre sure a mea ured with a, central venou catheter.
In many case fluid therapy can be reduced after the fir t 24 hours. us ually reducing the electrolyte and colloid lution to one-half of the initial amount. After the fir t few day the infu i n of ugar elution or fat ernulsi n for ba al metabolism is required. Caref u 1 ob ervation and measurement is nece ary to compen ate for individual. difference . The most valuable indication of an adequate rate of intravenou infu ion i " the urinary output. which hould be maintained at 30.-50 ml per h ur in adult and 1,5-25 ml per hour in children. A catheter i inserted into the bladder in order I, , m nit r the flow of urine accurately every hour .. Where the flow of urine i inadequate a 12.5 per cent oluti n of mannitol i ometimes recommended in order to initiate ali maintain diuresi and prevent renal. damage associated with haemoglobiauria ..
After the initial hock pha e, la ting two to three days and character! ed by 10 s of fluid nd oedema, the bum, wound, if they do not become infected, dry out and the oedema. begirt tosab ide. Thi i known a the re rption pha e and last from approximately the third to' the eighth day.
Moderate burn u ually require only three day of intravenou infu ion of fluids, For erious bums. infu ion may be reduced ucce ively, but the quantity and cornpo ilion of the fluid may require considerable variation, dependi,flg on the tendency to lungoedema. pneumonia and ep i . A new
h ck phase may occur due to heart damage or a cornbinati n of heart damage and fluid deficiency, Digitali 23 may be required where there are indications of heart failure. U line flow and blood pota ium and sodium level' require continual monitoring.
Maintenan eo/respiration
Maintenance f the individual' abillty to absorb 0 ygen i of primary importance. Administration of 95 per cent warmed and humidified oxygen, by mask or na al. tube, may be indicated if:
(a) there are bre thing difficulties (dy pn ea), a bluish or purple colouration of the kin and rnucou membrane. indicating oxygen deficiency (cyano i l or ound in theche t detectable with a stetho cope (rale );
13 Digilali i a powerful heart stimulant obtained [rom the dried leaves of Digilall purpurea (foxglove) plants.
170
(b) there are econd and/or third degree flame bum about. the 0.0 e or mouth;
( ) there i evidence that the patient wa overcome by rnoke r i re t·
Ie . con:fued or panicky;
td} the patient ha a cherry-red colour or was do e to a m uldering
fire when re cued, indicating the po sibility of carb n mono- ide intoxifica-
tion;
(e) there i. a hi tory of heart di ea e: or . .
if) the bum i pread over more than 50 per cent of the body area
(Phillip & C n table. undated).
Where the patienti breathing well on reaching the hospital,. oxygen may
not be nece ary even where there are bums around the nose and mouth , r orne possi.bilit.y of limited carbon monoxide poionin,g. The be t current mea ure of the patient' need of oxygen i the 0 ygenand carbon dioxide eeneentratton in the blood, whicb can be monitored by method which are available in rno t large ho pital . There i orne danger of oxygen toxicity from exce ive or prolonged use at high concentration .
Wheretherea;e ign of upper re pirat ry tract obstruction, Large amount of liquid in the re plratory passage or hallow breathing, tracheotomy-,the operation of making an opening directly in the "windpipe' 0 that 0 ygen can be adm.i:ni tered by tabe-s-may be required. Thi hould nly be d.one when it i clearly warranted by the ob erved symptom . ince tracheotomy may it elf be a factor in pulmonary infection (F ley, M ncrief & M son, 1968). 10 circumferential. deep burns of the che t it. may on rare cca ion be nece ary to inci e bum e char to permit
adequate che t expansion.
Treatment o/whitepilosphortls burn
Irrigation with a plentiful upply of water.immer ion in water or placing water- oaked pad on the bum urface top the combu tion of'ph ~horu in tantaneou ly ( rberg & Rosenqvi t, 1944). Often a cornbinati n of the e method. nun l be u ed, ince if the urface i allowed to dry the pho phorus reignite: . Although warm water i ometi~es recommended _it may be dangerou since it. can liquefy pho phoru particle (Mendel on in Curreri et al., 1970) and peed up ab orpticn making pho phoru penetrate deeper into the ti ue, Cold water make pho~boru. lidify. relieves
orne of the evere pain. and low the blood clrculatlon beneath and around the wound, thus minimizlns oedema and re ulting ti sue d~mag~. Water al 0' dilute acid formed by pbo ph oro . ombu tion. Phy ..• ologic • aline or weak sodium bicarbonate soluti ,0. i a better choice but eldom
available in large quaatitie in an emergency. .' .
The tanderd mean f ioWal treatment has been to irrigate the pho - phoru wound with a olution of copper ullph.ate, u ually a.t 5 per cent
171.
-trength {cr. NATO,,1958.; V:oenn,y.i Yestnik 48, Ma.y ~968, pp .. '$IS-lOW), which react, with tbe outer layer oftille phospl1oru particles to Form a dark coatilllg of copper phosphide which ,exdud'e- air, thereby prevenl.ingfiuther combu tioD of the phosphoru ' and he.lpililg to identify the particles,
In praetice, this tr,eatment has been disappointing (see below): moreover, copper sulphate is itself toxic and can be absorbed from the wound '(Sum~ merlin .. Walder, &. Monc~rief! 19~m. Whelan, Burkhalter & Gomez (1'968), report that thi treatment uneqaivocably caused the death of at. least one soldier with a 11.0 per cent bum. Thi mallcoUapsed with renal fai.I.llre after treatmem with copper sulphate for suspeered phophorus bums-a suspicion which turned out to be unfounded. Five of seven patient treated at renal units at the Cliark Alr Base in, thePfliUppinesand the Third Field Rospita] in Sawgoll died; the two survivors had not been treated with 'copper .. u~pbate at anytime.
Since copper sulphatle poisoning may be very similar to phosphorus poisonjng, the po ibitityarises that symetomsaueibueed to pho phorus in fact arise from the copper suWphate used in 'treatment. Accordingly thl que Hun is further examined lin chapter 4.
Since other methods are availabfe for detectingand inactivating phosphorus, ma;ny recent writers conclude that Ihere now aeemsto be 110 reason to place the burden of copper toxicity on patients allready threatened with phD phorus to,xi.ci.ty and other stresses of the bum wound (W:hel~an et ai .. 1 968}. Copper ·ulphalieis not very adequate as a mean- of excluding air and preventingcombwdon (Norberg & Rosenqvist. 1'944;. Ben-Bur. Galidi, Appelbaum & Neuman. (972). .. Norberg & Ro enqvist (1944) detected the luminosi~y of phospborus in the wound four bourafter vlgorou surgical, treatment with scalpels. and forceps, combined with the application of pad soaked iin 2 per cent copper ulphate, ,or 22 per cent. copper uliphate dis-
olved in glycerine. Copper .I:dphate was no more effective than irrigation with water (Norberg & Rosenqui t. 1944; Cuereri etal., 19'70).
To lnactivaee any re idtlalphophomsr,csistant to mechanical treatment, oxidiz.ingagents such as hydrogenperox.ide have been suggested! ,(Summer. lin etai.,1'967). Animal experiment have been conducted whi.ch how that a. Lper cent soludoD of potassium permaoga:nale in a 5 per cent. sodium bicarbonate olution neutralize the pbospholfiu. and remove all ncrroxidized elemental phosphorus. (Norber"g & R.osenqvist(944). Residual pho phorus ca.n be detected by mean off:1uorecence caused by ultraviolet lightir~ radiation (F.rye & Cucuel. 1969). Whelan et til. (968) report UUll lithium iodate-i opropanol is abo being inve tigated as a. pos ibl.e means of treatment.
Oth.er debridement compo ilion have been proposed for treatment of bums caused by variou liquefied whi.(e phosphorus mixture,. The e mixtures are considered to be more trouble orne thanolid white phospherus to remove from the wound urface. The cornpo Won recommended are
172
su pen ions of copper : ul:phate" var:iou . oils and organic olvents, or solutions of g~ycoerine, cop'per sui phate.,c tarehand detergent. (Rahinowitch, 1943; Godding & Nottcn, 1942). TiI.e u e of copper ulphate and organic solvents must be considered unwj e because of the deleterious effects IOf copper . alt and the risk of pee ding up ab orption of white phosphoru ' with the u e of Ilipid olvents,
In the face of certain techaicsl possibilities for "improving" white phophoru incendiary agent , which would make proper debridement. more tlme.-consuming, the aim of the treatment. must be fast removal of phosphoru (r,om the wound. This must be done with non-toxic so:lution which do not. interfere with other surgical wounds ali cause systemic poisoning or further damage to thetisue .
Animall experiments by Ben-Hut et til .. (197.2) ( ee al o chapter 4) showed that, with:inthe' experimental conditions. a solution of:5 per cent sodium bicarbonare and ] per cent hydroxy-ethyl-celiulose in :5 percent copper sulphate: solution prevent. both .y temicphosphorus and copper-poisoning.
Earlymorta:lity in evere chemical bm-ns is usuallyrelated to hypotension. and acute tubular neero is asa result of underestirnetion of the bum area and the depth of'tis ue necro L(Curreri etal., 1.'970). Thi underesthnatinn, in. combination with the possi.bi.l:ity of phosphorus absorption, makesflui.d resu citation and careful monitoring of urinary output neces ary, with
crupelou attention to erum edium concentration andserum 0 melerity.
The 6oHowhlg genera] trealment sehedale is recommended by theaathor cited:
I. Remove coataminated clothes andirrigare withlarge amount of cold water, or immer. e the affected part of the body in cold waeer, Care must be taken to maineain norma] body temperal:ure ..
2. A~W vjsible whii~e phosphorus partides should be removed with the aid of cal pel. forceps and pad - .. Phy-iologic aline or odium bicarbonate (5 per cent solution in water) should be u ed if available. Thi treatment is extremely pa~nful andi best done under anaesthe ia,
3. Inten e mechanics] treatment under irrigation or immersion with a I percent" ta iurn perrnanganate in 5 per cent odium bicasbonate solutimil· hould be performed ulltiW lumino 'it.}' or t1uoresc,ence ceases, indicatling that all the whitephosphore ha been nelJrr9J.lj~zed.
4. Padsoaked with the permanganate soliutionhould belen en tile wound forome hours.
5. .. In case of occular injury irriga.tion . hould can i t of water or pby lological saline for at least balf an hour. No pads bould be placed on the: eye since it Limportan.t. to maintain i[mobm~y.
6 .. Further treatment continue . as for thermal burn.
n must be emphasized [hat this trealmellt.i to be carried mill[ wW'1. ut delay irf the risk of pho phoro poisoning i to be avoided. Tbus, correct treatment in battlefield condition demands sub tent:ial medical faciliries,
In
The prevention and treatment of il.r/ec.tion
The prevention and treatment of infection include the f Hawing three rneasur : (a) the reduction. of ource of infe tion by a ep i in the patient's environment b the treatment of the bum wound itself to prevent infection ( ep is) f the wound and ( ) prophyla tic and curative measure to prevent g neralized infection of the body y tem epticaemia) resulting from rnicroorgani rns and toxin in the circulating blood ..
Asepsis. The need for complex and through aep i • i . particularly irnportane in the treatment of bum wound. Mea ures include not onliy u! ual precaution of iterile clothing cmbbing, masks, glove .. and on for medical per onnel, but preferably treatment of the patient in an .i elated
terile chamber well ventilated by filtered air.
A further mean of reducing th threat of bacterial infection i ultr violet irradiation. U ually thi require the provi ion of an ante-r om. provided with ultraviolet lamp. through which all taft' mut pa before they reach the patient' i lati n room. Considerable ucce ha been reported in reducing infecti.on by such means (Hart 1936; Hart, Po tlethwan, Brown, Smith & John on, 1968).
A noteworthy improvementin reducing infection wa . a bieved by Colebrook and hi colleagues at the Birmingham Accidene Ho pital, England. t ward the end of World War It Dre ing were changed in pe ial a eptic chamber devi ed by B urdillon entilated by ab ut 30- cubic metre per minute f warmed, twice-filtered air. hi rapid ai.rflow carried with it out of the cham r particle and bacteria liberated from the patient' dre 'ing which might otherwi e have c ntarninated the new dre ing (Bourdillon & Colebrook, 1946). Thi approach ha been developed in recent year. me promi ing result have been obtained with a pia tic ventilated il olator. The i . lat. r is a large, tran parent box-like con traction in which the patient lie .. The patient an thus both be readily obervedand have the opp rtumty to ee out. which may be p ychologi ally beneficial in contra t to i alation room . where the patient i observed by television camera but may suffer from la k of cial contact. The i olat r i quipped with glove port and [ran fer pouche on both ide f (he patient. ma.king it po ibl to treat the patient but protect him fr m ontamination by contact. Or fr m th air
Hayne & Hench, 1965; Lowbury. 1967' . evitan, Seidler, Strong & Herman, 19
Another meth ell has been developed where patientsare treatedini alated ro m through which filtered warm dry air i pumped ntinuously (Liljedahl. 1971). This air i warmed to 32- 6°C and it humidity i controlled. Medical per nnel mu t pa through an ultraviolet irradiation chamber before entering th patient; ro m and the patient i mainly ob-
erved vi t levi ion earner and th r remote mean. ]11, this meth d, not nly i the patient pr tected fr m b teri in [he air, but the warm, dry
174
Tllble 3.17. [)eellne 101 mortality foUoWing treatment. or bum wounds wUhmafenide eetate
With topi al therapy (1964-1970)
Percent of b dy burned
0-30 30-40 40-S0 50-60 611-100
4.3 44.4 61.1 7 .3
9.1
_.0 12.6 23.1 411.0 79.
Source: Pruitt &: Cum:ri 1971).
air rapidly drie out the open wound which form a protective cru t in a few hours. This ha enabled an open method of tre trnent to be developed, in contrast t the traditional clo ed method of covering the patient with dressings. The patient lie all, a pecial bed enabling him to be turned without being moved from t.he bed. The bed i covered with a sheet of aluminized fibre, which doe nor adhere to the wound and in addition provides a certain protection again t infection. U e of thi method avoid tile conunual change f dre sing which are a. major ource ofexcrutiating pain to the patient. Very few of the e patient develop Pseudomonas infection which ha been a major clinical problem (Liljedahl, 1967 1971; Coriell Blakemore & McGarrity 1968).
Medicinal treatment of the wound. There are tw reason why uch measure a tho e ab ve are notufficient Fir to even with the rna t elaborate facilitie , orne case f infection occur .. econd facilitie uch a tho e de cribed above are 0 elaborate and so ctly that (hey are imply not avatlable in mot areas of the world, or are not available on a cale applicable to large numbers of battle casuatues. The development . f': urface mean of tre tment, uch a antibiotic cream whi h can be. put n the wound •. i theref re f c nsiderable imp rtance.
During World War J a 1 cal application f picric acid wa u ed t treat bum wound. David on (1925) introduced the u e of tannic acid in Detroit a method. which remained c mmon until. World War II. Bum casualtie at Pearl Harbour and at the Coconut Or ve night club fire in Bostont' were treated with intraven u inject.ion of sulphonamides (Evans & H ver 1943; Cope, 1943). Later, ulphonamide-penicillin and penicillin cream were used for local appliceticn, beforeappliying a dre jing..
More recently a group at the US Army In titute of "urgical Re earch
s. n 20 November 1942. 491 people died in a lire at a 80 ton. Ma_saehuseu nightclub. The Massachu eus General Hospital received 114 dead and injured. _ cia lc erie of papers
on these ca W3 published in the Annals of IIrl/'i'f)' 1 n 16) 1943.
1.75
has developed an antibiotic cream, contajning mafenide acetate •. known a Sulphalmylon, which has resulted in a considerabl1e decrease In mortality (table 3.17) (Lindberg, Moncrief. Swiltzer, Order & Mills, 1965; Monc:rief" Lindberg & Switzer,1966,).~ This treatment .i ., now widely used. Mafenide is, a methylated SUlpha compound Which" in the ~orm. of the acetate salt, i suspended in a soluble ba e. Tbws-uspension iSl'egardeJdas cliiticaJly important in order to permit continued absorption into '!:he eschar and maintenance of effeetiveeoncenteanens ofttle medicament at the level! of the interrace between the viable and the non-viabl.,e tissue-tbe ,characteristic . i.ie of bacterial plrOlifer.ation (Pruitt & Curreri, 19'71). Mafenide acetate cream is a bacteriostaeic rather than !II bacleriocide;thal is, it does not
terilize the wound by des troying the bacteria but it. prevents them spreading and infecting non-burned tissue (M.oncriefet al., 1966.) .. Mafenid.e acetate cream i pread over the entire wound with a sterile tongue blade ora ter:il!e gloved band. following daily cleansing, wound debridement, phy iothera.p.y and hydrotilerapy carried out in apecial tank ,(Hubbard tank) in the ward. Twelve hourslarer the cream. may be reapplied to. areas where it ha been removed by contact with the bed clothes.
A number of side effects have been noted with U'l.e use of mafentdeacetese cream. The cream causes some initial pain and discomfort to the patient, Hyper ensitivity reactions occur in some 7 per cent of patients (P:ruiu & Curreri, 11971). More serieus i . the development of respi:ratorycomptica~ lions due toin_hibition of the enzymecarbonic anhydrase. which is responsilble for t:he normal proces of excretion 'of carbon dioxide fli1lm the blood into the air to be exhaled from the lungs.26 Ma:fenide may al 0 de~ay epitbeJj~ization ..
A second mean, oftopicallt:reatment. which has been wide~y used in reeent years is the .applicationof thick sterile dres ings soaked ina solution ef 0.5 per cent liver nitrat,e(MonllliFo' &; Moyer, 196:5:P'olk 1966; Polk. Monafo &; Moyer, 1969). Hypersensitivity reactiens have not been aUr~buted to the use of this, agent and no development of resistant organisms has been acted. It i .. most ,effectiVe when applied within 24 hour of the injury, and isactive against the entire spectrum of wound bacleria,.allhough ome cases ofctostridialmyositis have been noted (Monaio',Brentano &; Gravena, 11966). On the other hand, ilver nitrate doe not penetrate a deeply as
U A,rt,hur D. Mas~n. Jr., and Ro'berl B .. Lindberg won thel97Z US A~my Research and Development Achu~ ... ernent Award for their dlscoveryarul development of SulphamylO!l
cream (.US Army Medical Department Newsletter 4 0). I 97.2}, .
~ ··Alve.olar"arte:ri~lcarboll d'ioxide gradientset' significance jtave been measnred fn patle_nlS wltb elNenSlve burns who have elevated serum levels of mafenid'e, acetate and ilS, pn",lary 'breakdown prod'uct P-<:lIrboxyben2iene sulfonamid'e. In such a situation upervemng p~~onary complicalion.. rurth.er interfering with carbon dioxide excretion, ~ay caus~ ~p!d change frem respiratory alkal'osis to acidosis. The mafenide acelatec~eam s_ho~d !hen. be removed From thelium wound and bufIluin.s earned our as necessary" (1f'l"um & Curr,eri. 1971, p.464).
mafenide an.d requires theapplh::al:ion of thick. occlusive dressings, and on eontact it disc.olours not only the patient' unburned-kin but bedclcthe and aUend:in,g personnel a, well. .A number of ide effects have been. reported"induding deficit of electrolyte (odium. potas i:umand calcium] methaemoglobinaemia. 1(31 farm or bl:oodpoi oning), and a re triction of the movement- of joints., due largely 10 the dressings. (Turnberg & Luee, 1.'968; Polk, 1966).
The Chinee news agency Hsinhua reported 011 8 August 1973. that the teaching ho pital of the Nantung Medical College in ea tern China' Kiang u province ha treatedextensive burns with a herb, Itex cldn.ensis sim (a species of hoUy), for over three years withgood effect, The herb had been used by practitioners oftradjtienal Chinese :medicine for many years. Topical treatment of the wound with a solution or cream containing the herb had an anfibacterial eneet, confirmed by bacterial cultures from 60 patient on 240 eccasions, and had the advantage of rapid ~orma.t[on of crusts on the wounds, little exudation, slight infection, rapid healing and few compUcations. By preventinga large amount of exudalion,Duid requirements wereel 0. reduced. In addition the herb has the advantage of being aburrdant, inexpensive and easy tiO' u e.
Other recent jepical treatment include gentamicin ~ ulpilale (Stone, 1966).. suWphadiazilneilver cr,ea:m(Fox,. Roppole & Stanford. (969) and variou silver creams (Butcher, Margraf & Gr.avens,1969).
Burn wounds may also be infected by fungi. ueh as Candida, and by viru es, such as Herpesvirus hominus, Sy temic antifungal. agents have not been particularly ef'fecHvein combating fungal infection and the infected area. may have to be removed urgically, However. topical application of nystatin. (Myco. tathll)is being evaluated in the laborawry (Pru~n & Curreri, 1'971).. Several. patients have died due to H. l!omirw,s and post mortem examination ha .. hown systemic le ions in the oe ophagus, Ilung., gastreintestinaJ tract .and liver. Since no adequatemeaas of treatment is pre ent]y availabl.e it is fortunatethat most vb-aID bum woundinfectiens do, nol spread in this way. Topical application of idaxurid~l1e is being inve tigated as a therapeutic measure ,(Pruitt &; Carrera, 1971).
Ge1l:eral prophyiacUc mea ures, In addition to direct treatment of the wound. mea ures to prevent general bodily infection by bacteria and their toxin may be required, Threegeneral approache are available. The first lis toreplace the deficil in the body's natura'! mean of defence by adnlinJtration of replacement of gammagl.obulin... he second approach i . the ad mini tration ofantibioli.c drugs uchas peniciUi.n. The !third .a.pproach lis the adrnini tration of a vaccine.
LiljedahJ (1967), recommended that the propllylacticadmlinislrati.on of 20-40 mI of a 12 per cent. solution af human gammag]obuHn be adminis tered between the third and the eighth to tenth day after (he bum ilojiury .. No definite clinical eenfirmation of it effectiveness had been re-
13-7431.68
177
corded, Ithough Birke et al, 1964) previou Iy dem nstrated the, con-
iderableinitiallo of gammagl bulin and a rate of breakdown five to ix time the normal rate in burn-injured patient. In the four year of con istent treatment wiith gammaglobulin mortality due to infection decrea 'ed con• iderably, although other factors were al 0 involved.
A in many pect f the treatment of burn there i orne variation in medical opinion regarding the u e of antibiotic. Many authritie agree on the value of prophylactic penicillin do es of from 300 000 to one rnilhon unit a day for alii patient with igni:fieant bum (Philillip & Con table, undated), Thi applies particularly to patient withpulmonary complication . How ver, antibiotic are n ub titute for meticulou wound care. In parti ular there i a danger that general antibiotic treatment may change the b cterial flora of the wound 0 that if pticaemia develop later it w,jU be fr mall organi m resi tant to normal antibiotic . There i a trend away from prophylactic antibiotic treatment in many burn unit (LiJjedah]'I'967). and the re ervation of antibiotic for the treatment of infection due to
pecific, identified organi m i recommended (Phillip & Con table, und ted).
Alexander & Fi her (1970), report the development of an antigen vaccine again t Pseudomonas bacteria, a major cau e f death from bum .
kin, grafting
The fir t stage in the surgical! treanaent of the bum wound i the removal of deadtis ue, In orne case dead ti ue may be remov d by crubbing (Litvine, 1970) r wa hing with a jet of water (US Army Research and Development Nell • Augu t 1972. In other ca e urgical e ci i n i required. WbiJe orne author (Jack onetal. 1960) advocate earlyexci ion this procedure i perhaps to be preferred onIDy in the case of clearly delineated deep bum covering Ie than 5 per ent of the body (Backdahl, Liljedahl & Troell, 1962). Other auth r recommend e i i n after _O~25 day. when it n l e carried out with con iderably Ie 10 of blood (Liljedahl" 1967).
The ultimate obj ctive of all bum wound care' i to replace the 10 tskin a' oon a po ible, Alth ugh the skin may regenerate it elf, in a fun thickne burn it does only at the edge f th ound, here the oldskin remain intact. In large third degree bum , the rate f regrowth f the
kin may never be sufficient to cover the wound. For thi rea on it i nece ary to re ort to urgical mea ure to replace the : kin. foil wing clean ing and preparation of th . wound.
In order t er the large bum w und piece of kin are tran planted
from other area of the b dy, a procedure kn wn a autografting. he rn t ommon techni.que L to remove" plii.Hhicklle" kin from a donor ite with a special instrument. The plit-thickne graft is a thin layer f kin
178
hich include the epidermi and part of the dermi but leave a ufficient depth of dermi _ t enable rapid degeneration. During thi period the donor
ite is an additional ouree f pain and di comfort and may it elf become infected. For thi rea o III urgeon working in primitive or combat onditions may prefer not to tran plant. skin, e ell though they may b techni ally competent to do o.
unetional and c rnetic c nsideration dictate pri rity to area uch as the hand. feet, joint and face. which hould be covered before nonfuncticnal urfaces, In patient with exten ive burnsand limited donor siee . "me hed" autograft may be used (T nner, Vandeput &. Olley, 1964; Stone & Hobby, 1965). In thi technique the kin i perf rated by a erieof mall cut 0 that it an be drawn out into ... lace" or "net" up to nine time the original area. The inter tice fthi me h regenerate rapidly. However. tile re ultingkin i ant co rnetically ati factory and i thinner than n rrnal; thu the technique i not recommended for the face or for joint, feet and other rea expo ed to on tant wear (Pruitt & Curreri, 1971).
It may t ke everal month of kin-grafting operation toe vel' an extensive bum. ince the patient will have little rernaining kin to donate to the burned area. In uch ca: e ucce ive "crop ... f kin rnU t be tran plan ted from th . arne healthyarea _ . Becau eft hi problem, everal other material have been u ed for temporarily covering the urn, including
kin from other per on or animal. and ynthetic material .
The first clinical use of animal kin graft wa descri ed in the eventeenth century and the transfer of tern porary kin graft_ from one person t: another wa fir t re orded in the nineteenth century (Davi . 1910). kin graft from other per on may betaken from adavers, amputated part or living vclunteer , in [hat. order of preference (Pruitt & Curreri, 1971.). Such pieces of skin may be treatedand kept for a hort time under refrigeration. They will. erve a acceptable dre . ings for up to two week .
Le ati fa. tory but al 0 acceptable are graft fr m dog (Switzer. Mon-
crief & Mill , 1.966 and pig (Brarnberg, Song & Mohn, 1965). Pig kin graft treated by electron-beam irradiati n may betored under refrigeration until needed. Thee graft are more diffi.cuh to apply and how les adhe iv ne . They may have the advantage f being more readily available. at Ie t in the ca e of pig kin .. which can now be obtained commercially. Vi hnev kii (1966) report that fr g kin ha b en used in the arne w.ay in [he Democratic Republi.c of Viet-Nam,
A.yntheti.c polymer burncovering ha recently been describ d by Gre-
gory, chwope & Wi e (t 973).
The common u e of u h temporary "phy iol gical dre ing .. are given by Pruitt & Curreri (1971) a follow _:. (0) debridement of untidy wound. (b) protection and "stimulation" of granulation rissue following
schar ~ paration, (c) immediate verage ofe ci ed bum wounds, Cd)
179
coverage ,of ,eschar-free bum _ between autogmfiingpJloc,edures inpatients with large bums and limited donor sites, '(e) as a "let material" to determine lI'eadines ' of fIlU-thic.kllless, burns to accept an autogreft of the pati.ent.'s own , kin" and 00, provision of ~emporaliY coverage for any oUter urgical wound whichcannot or should not be closed immediateliy.
Tbeapplication of temporary graft- decrea e the 10·s5 ·of water and heat by evapuration.and dimini hes the exudation of pr'otein and blood. Wound pain i -trikinglly decrea ed, par1icularl:y in clillUdren wi:fh the decrease in discomfort enhancing the use .of joints, thus hel,ping toensure maximum functional lie ults (Pruitt & Currert, 19'7]; Shuck, Pruitt & Moncrief. 1,'969). ..-
ReCOfWrllc1i1l1? sllr-g,ery (mel rehabilitation
Burned tissue of the hand, face and neck, which is particularly common in war burns casualties, i the mot likely to resuh in di.sfigurement and flJl1ctionalimpairment, the most. difficult to recon truct.and the rno t e ential: to normal social life. One .' f the leading pedaUsls on the recen truetion of the face after bum deformiti,es ha u~mariz,edthe situation as follows:
llillhe, face and neck. contrac I 1.1 re and SC<lJr . the re uti of tissue de truction from b~rn • dj .. tort t~e SQ~tli slIe structure and may resulr :j:n evere facial disfigurement ~.1ild functienal trnpamnent ... The J1eCOIl nructive urgica] r,ehabililation of the patle~1 who bears seersend centractures following burn of the face and neck i a ~~~?~ ta,k for the pl'a_lic urgeon .. A important asthe ndief of functional disabll:IU,e_! the reduetton of the severity of facial disfigllrement and its attendant socIOIO,gl~~I, psy.chologjcal, and vocational. implication' (Conver e,I967, p ... 323),. _ The I~IMI pe,:od O~lreatmelll in the hospital ha cOllcentratedupon the ensarance of survival; facml d.lisfig;uremenl: now becomes a major problem if conrracmre . and.hy~ertrophic c~ marl~e paliellf . facial features ... The rerum ofa p-ati~nt 10,hJS hom: after a long period of hospitaiiz.ation may be atraumane experience. It tse sential that the patient be forewarned of the reaclioll of members of the fa~liIy. friend. and neighbours. A thorough understanding osthe part .of the patient' . s,pouse and other member of hi family is equalliy important nile of our pal~~nl~ recall t~a(, ~hen he returned home hi two children recoiled, creaming, at the Ight of their di figured father. (lbl~d .• p, 333)
In these circumstance iti understandable thatthere j olflena clamour for earlY treatment. But the surgeon must res] t the pre 1JJre placed upon him both. by the patient and the family to. undertake early reconstructive procedures, ince t:ime mu t be allowed for the maturation of the . car ti sue and metabelic aad immul1ol.ogiCaJlalbi~izaliol1,aR~er the severe
train which have been placed upon 'the normal phyiological functions of the body (Converse, 1967). Mathew' (1964) report thatthe besa re ult were obtained in repatriated pri eners of war who had had 3. forced debw of per hap two years before recce tructive urgery could be undertaken.
A few other genera] poinl- may be made alb ut the problem of reo constructive_urgery. Early skin grafting is generally recognized to reduce
180
the problem ofhypertflo,phic earring aadenntraettons, but not to remove it. The mo. t common type of graft In current practice, t.be split-thicknes kin graft contracts both during and after the peri.od of healing, The younger the patient the greater the amourll ofeolltraclion.
Hypertrophic car iare al 0 more common ill children:
The propenslty of chj'ldren to hypertrophic car; i. well known and s'im:ilar scar OCCL!ir ill doncr area. followinG the removal of split-thicknea 'kill graft of exeessive thickness. In the child, theskini relativdiy thinner because it is distended everasubcutanecus adipose layer which i thicker tban in the adult and penetrate into tile base of the dermi through larger and more numerou "columnae ~Idiiposae" (Collver e, 1967,1", 332),
Hypertrophic: scars can occur in various areas ofthe face. There an indication thatcertain individuals or racial types, may be more predisposed than others to 'lJcb scars, although the .tate of nUlrition and general health arealse determining factora, The most seriou defnrmisies occur in those patients in whom initial kin gr.aftin8 bas been delayed or unsuccessful.
Afiter at waiting period to ,enabl~e :uch sears tiO stabilize, the dlifticult, tedious. drawn-outand costly process of'reconstructive surgery caD beg]D.~7
For the palielll" thenumeroua and repeated operations may repre enta test for the most eaurageous ... Because of the often protra.Cled, period ot'treatraem and nuraeroua operations.,lheimporta:nce of the p ychological management of the severely bumedpatient lis obvious; most of this management will re lllpon the
urgeolll in whom the patient lills placed hi confidence and who mast ala act as his psychiatri t (Converse, 11967 i p .. 336).
One illustration of the length and tediousness of'the treatment is the problem. of preventing eentractures of the neck after corrective surgery, A great advanee in the treatment of ucb contracture was made by Cronin (1957), who put his patient into. 3. m.oulded neck splint after kin gJafting. Thi . splint had to be worn. continuously for five t~o six. months. Deformities around the eyes are particularly common, due to the thin tissue of the eye lid .. Further, the eye are particularly liable to infection after bum ., Re idual car pre ent di!fficulit problem. in the final tage of rehabilitaoon. The removal of these cars, where pos-i.ble,i p ychol~ogically benefi.cial. to the patient,
U Dr John ConsUlble. plastic surgeon: all.he Ma achusetu 'General Ho ,pila!. Bo ton .. Ma ' .. estimated thai thecurrent C05t of such a hospital Slay in the United SJ31.es may be a much as $100000. Tile running, co ts of treatment at the bum cllnic 8't the Karolin ka. Ho pital in Stockholm were Sw. e-. il 018000 ($2$4'000) in 1972. The clinic reported 3, :147 patient-day of treatment, Uta.t is. an, a .... e.rnge of 8-9' palients al. any lime. which! gives :8 dajJy cot of Sw.cr .. 323 . .5($80') per patien:t .• The treatment period r.rmged from amin . Imum ot I. mont!! til' 8-9 month. giving a trealm.cnt cost of Sw, er .. 970S ,tSc240();) to Sw..cr. 87345; ($'21700),. Tills includes staff alari.es and, medicines, but not overhead co ts such as rent, electricity, heal, :~ood, ad:mini tralion •. and so on. Thus Ute Itotal costs are even higher.
181
V. Additional military medical con iderations
The foregoing ection de cri ed me of the ba ic problem in the treatment
f bums, ba ed on tile be t method' available in ideal conditi n . In combat conditions. the treatment of bum .i complicated by a ciated mechanical inj~~i~ from bla t and fragmentation weapon, and by limited or damaged facilitie . The state of nutriti III and of public health of the population affected by incendiary attack are ignificant fact r in their U eptibility to injury.
It i common military practi e to u e incendiary weapons in combination with ther weapon. uch a m hine-gun and fragmentation grenade .; population centres may be b mbed with a combination of high explo ive and incendiary b mb . A a re ult, many vi tim may suffer from both bum wound: and bla t and penetrating wound . In orne ca e . uch a an exploding white phosph ru muaition, the pastide of incendiaryagent may themselve au e multiple penetrating wound (Pruitt. 1970. Thi hazard may be increa ed a re earch continue into the deve] prnent of "reactive fragment " ( ee chapter 2).
Experimental tudie have demon trated that combined injurie from thermal and mechanical trauma may cau e a much greater rate of death than either form. of injury al De. The mortality rate in mice following mechanical injury with a normal death rate of 10 per cent wa increased eight-to-tenfold if preceded by a. sublethal bum injury 0-3 dayearli.er ( childt, I 972).
Table 3.18 . hows the propornon of bum cas es ' ufFering from additional injurie treated at. the US Army In titute of Surgical Re earch between 1965 and 1.969, which include injurie incurrediin both combat and noncombat condition. In the majority f the e ca e the bum were inflicted through UI.e igni.tion of fuel in combat vehicles rattler than by incendiary we· pon . Even o, it j apparent that bum resulting from ho tile action are more serious than tho e frem accidental event. A tudy of 1963 burn patients
Table 3.18. Burn patients with assodated lnju.ri- . Bdmitted to 'he. US ~rmy InstiCute of urgical Research 1965-69
Patients with associated inj I.J rie
Total burn
Year admission umber
1965 174 20
1966 II 67
1967 389 96
1968 389 106
1969 01 80
~otal W 564 369 per cent of total
11.5 2.1,6 24.7 27.2 26.6
2:3.6
Srmf e: Pruitt (1970).
182
treated ata US Army ho pital at Yokohama, Japan. howed that hostile causes accounted for 43.2 per cent of the hospital admi ion and 69'.3 per cent of the death. while ccidental au account d for -1._ and 30.7 per cent, re pectively (Allen. in DiVicenti et al., 1971). The c rnbat casualtie. in. mo tc se the trapped crews of armoured vehicle f helicopter 10 ~hich the fuel exploded were u ually m re evere and as ociated with mechanical illjurieandl i.nhala.ti.on injuries due [.0 large amount of rnoke and car onaceou product, It i likely that the combat u e of napalm together with. corrventional munition createsa omewh.atimHar pattern of
injury.
The treatment· f the bum wound by method uch a 1.1:10 e outlined
above i in general c mpatible with the treatment of a ociated mechanical illjurie . Conver ely, however Pruitt (:1970) conclude that t.h~ ~re ence?f bum in the multiple injury patient greatly increa e the po ibility of epuc ,complication and necessitate modification in many of the standard urgi-
cal technique a.nd principles of wound care. .
A second factor of gre'at importaace in combateonditionsi the general tate of health and nutrition f the populati n at ri k. The pr gno i for a burned patient. I highly dep ndent nof. onl.y upon hisage, a noted earlier, but upon hi general phy leal. condition. Per n with anaemia or a I w tate of nutrition have greatly reduced ability to urvlve a evere bum. In ome war a ub tantial part of the target p pulation may uffer fr rn food shortage. either a are ult of their tate of economic development or a a
result of the de truction of food upplie or mean of di tribution.28 A low st te of nutrition not only increase the death rate from burn butal 0 make wound more difficult to heal and more liable to hypertrophic
earring and ther forms of di figurernent,
]n wartime condition. the pos ibilitie for optimal treatment are often greatly dirnini hed. Wide pread u e of incendiarie may re ult in a rate of bum. ca u hie far greater than can be coped with by availa le medical facilitie . Indeed, the e perience of civili nair crashes how that the bum treatment facilitie over a wide area may be tretched to their limit by an influx of, say, some 50eriou ly burned patient . In military medicine fine judgements. may be required concerning how best to uti1iz limited re-
ouree (Wallace. 1969 . .
The problem of limited re ource i highlighted in twotype f warfare in which incendiarie have been widely u ed. The mas de truction of ad-
ughterson & Warren 19 6) report that to' ards Iheend of .'?i: war in J8pll~~ ,"the inhabitant. or the citie were seri usly undernouri hed ... MalnUtrition wa resp m Ible ~or many death among injured people already weakened b u~demourishmenl .. , ,. HI. .1). Dudley et al, (1968) 'IY "our experience lead us to believe thllll the outhea I Ian eivilian. perhap because f marginal subnutrition, p. rhaps bec.:mse of om~ lIn?c!!: 11:,([ specific deficien y ha inherently les ability 10 respond 10 mas rve trauma than either hi litter. betler·fed! military counterpart. or the. Westerner" (p., 339.
I. 3
vanced indu U-ial citie by the combined u ed of incendiary and high e plo sive bomb not only create many casualtle , bUI. a1 0 destroy a large proportion of the medical facilitjeJ which tend to be cone ntrated in these area .29 In the econd type r combat ituati n, ineendiarie have been u ed again t guerilla liberation armie in area' which only p e the mo l rudimentary medical facilitie . 30[n neither ca e i evacuation from the theatre of operati n a po ible elution ~o the problem of limited medical re urces, and nly irnple f rm of treatment can be attempted .. , By removing any h pe of adequate treatment. the uffering of the burned per on i magnified, ince the pr blem of treating severe bum wound become almo t in urmountable. V,icrim will either be left to die. r if they recover from le er bum. they will be left to cope with their own di abilitie and disfigurement ,including in orne case open wound - which never heal.
In order to make a c mplete humanitarian a e ment of incendiary weap n It 1 nece ary t con ider aU the e aspect of the ircurn tance in which they are used,
2J! Oughrer on &. Warren (1956) report rhat "In Hiroshima, rno t of the medical facilitie were in the devastated area. and the larger part of them wereextremely vulnerable 10 bit and fire: con equently ca uahie were heavy, Ninety percent of the 200 'to 300 physician were killed or injured .,,, Jmost every hospital in .Hiroshimawi'lhin I mile of the hypo-
enter was 0 severely damaged that il could nOI. function as a ho pital, nly 3 of the 45 civilian ho pitlll were u able" . ,," IP'. 71 m. Morerecently, e len ive damage to hospital in North Viet.- iam has been! well do umerued (US - ' nate Committee 00 the Judiciary. 1972).. h i undear from the publi hed in~ rmati n on target . election hether uhese attacks are tho: re 'ult of Irnpreclse v'preci ion bombing" r precise attacks intended to un~ermine mor~I'e. The problem hastn any case reached . uch proportions, thaI the International Comm!l~ee of t~e Red res (19730 1 i eeking 10 strengthen the provisiensin the
Geneva nvenn ns de igned to protect medical resources from attack.
30 The medical service of the ational Liberation -orces of Yuga lavia, for example, had to f ce (he .foll ,,\ ing pr blern during World War U: "Doctors h d [ nee as refugee r fac.e death. Imp~ onmen! or deportation ... The German eerned 10 have made II special polnl of de troymg hcspltals, or any other building capabl of being u ed as uch.". the enemy n many ceca ion slaughtered all the patients and Sluff they captured before de-
[raying the hospilH!. Under such circum lance the wa tage of medi :al per onnel, scanty to begin W.ilh, was enormou ." 'tHir I, 1945, p. 1(6).
More recently. a 'lB'1f report prepared for the subc mmhtee on refugee of [he U enate ommittee on the Judiciary (1970 . de cribed bombing raid in Lao. with as many .BS 600 planes II day, dropping napalm. pho ph ru . antiper onncl bomb and high explo ive bomb and concluded Ihat'"with a very low tandard of medical care generally, and with a near totul absence of adequategovernment hospital" the burden of war casualty treatment in Lao is "pecially heavy" (pp. ]2-). report prepared by 'the General ccounting
[fice of the U enate e timated that there were "about 36 Laotian doctor . of which
I: are in the military and .19 are adrnini strators orlhe R yul Lao G vernment" (Collgres-
siona! Re ard.] lay 1972). ceerding to Webb (I I. a former surgeon lit the
John F. Kennedy enter f r pecial warfare, the "denial of medical resources to in'urg~~! .. i an important facet of counter-guerilla warfare, It i noteworthy thai the Draf) ~ddjIIOM~ Prot ols10 the Four Geneva onventions of 1949 contain the paragraph:
In n crrecrnstance shall any p rson be puni hed for carrying oUI medical activitie compatible with pr fe ional ethic . regardless of the person benefiting therefrom." UCR • 1973a)"
184
VI. The question of uffering
The purp of thi chapt.er ba been to de eribe the mode of action of
incendiary weap n n the buman b dy. Thi mode f action I com ple
and depend.ent upon the circum lance of th bum, the deptb and e tent, the part of the b dy affected. the pre ence of other il\iurie . as wel~ upon the age and e ndition f the victim. and the quality of the medical
re ou rees available.
Military incendiary agent in genera] cau e deep and exten ive burn ,
ine they have been developed to the level necessary to ignite or damage materials, uch a metal. much m re durable than the human body. Further, their u e is typically combined with explo live and fragmentation weap n mutually t enhance the effect.
The medical treatment f evere bum uch a tho e caused by incendiary weap n i more eo Uy, difficult. tediou and demanding both for thepatientand the medical taff thani treatment of most other type of injury or iekness. Such tre ttment i not likely to be available to the maj dty of incendiary casuakies, either in rural areas, or foJlo,wlng trategic incendiary or nuclear attack on citie leading to mas casualties.
Th victim of a very eriou burn doe not nece arily d.ie immediately.
He may live for II ur , days, or even week, depending upon the quality of the acces ible medical treatment ince even a large area of damage to the kin d e not have the immediate impact of. ay, a bullet wound in the heart or brain. Death follow. in due cour e from infection, rom the complex. pby lologicaleffect of hock consequent upon 10 ffluids, fT m respiratory complication • or from ub equent train on other organ leading t heart, kidney or lung fai,lure. or ga tric or duodenal ulcers. E cept where exceptional medical facilitieare available n uch a grandcale a are found in only orne ten of peciali t bum unit around the world. the death of the victim of seriou bum is r ndered probable •. if not inevitable
but. not neee arily rapid,
The victim of deep, third degree burn may uffer Httleimmediate pain
ince the pain receptor of the kin are them elves de troyed. The patient may even die witbout feeling much pain. For tho e who urvive and for tho e with areas of Ie severe bum; pain i e eruciating, inten i.fyingver a long period during recovery. Deep bum require kin tran.plantation which i~tself reate painful donor ite on other areas of the body. In many part of the world uch e ential urgery may not be undertaken either be au e surgical facilitie are not available. or beeau e the don r sites may them elve bee me a . ource f infection. In the e circumtance ,. the bum wound may never heal, placing the patient under permanent threat of infection a wellas under an enorm u p Y hologi aJ burden.
The can titutron of the W rid Health Organization (WH.o) define health
a • a. tate of phy ical mental and cial well-being and not merely the
t.85
ab ~nce of disease odnlikmJI.y': Suffer.ing may be defined by the converse a "a state c,r phyical,. mental and social distre • and not merely the pre ence of di ease or. infirmity.' . ~ere can be no doubt that incendiary weap~n cau e exce ive uffering In the fulle t en e f thi definition.
In v~ew of.the e facts, the verdi t of the Special Committee of the League ~f Nation di armament conference in 1932 wa that "the cruelty inherent In the uses of the e ~~plianc,e [cause] ulfering that cannot be regarded a neces ary from a mlhtarytandpDint" ( ee chapter I ). U i , difflcult to ee
any rea on to rever: e thi judgement. -
186
Chapter 4. 'Toxic effects· of ineendiary weapons on the human body
I. Introduction
Wben. material are burnt or decompo ed by heat, a variety of ga eous, liquid and solid sub tance are produced, Many of the e ub lance particularly certain gase and make made up of olid particles or droplet: of acid. have toxic effect which in certain circum lance bave provedto be tbe predominant caue of' death and injury re ulting from fire. Examples of toxic agents produced by Dr in fire include phosphine, hydrogen chloride, hydrogen cyanide, phosphoric acid, metal oxide and carbon monoxide. The toxic hazards of fire can thu no longer be overlooked either in the civilian or in the military context. This chapter review a number of the products of combusdon or thermal decomp ition of incendiary agent, and considers the toxicity of these products ..
Toxic effects may al .0 be produced by the direct action of certain incendiary agent on the human body. Recent clinical and experimental tudles have hown that white phosphoru may be an agent of thi kind.
Theavailable literature on the toxicity of white ph phoru burns hasbeen exten ively reviewed in appendix 4A.
In .appendix. 4B the toxicity of various incendiary agent and product of combu tion are, presented.
II. Incendiary agents as a phyxlanl
Oxygen i essential both for human Life and combu tion. With theexceptlon of the pyrotechnic incendiarie ,(which obtain oxygen from an oxidizin.g agent in the compo ition) incendiarie draw oxygen from the air. Where the.uppl.y of air is limited, as in a building, insufflcient oxygen may be available to ensure complete combu tion, while at the arne time a variety of potentially lethal and toxic product may be generated.
In exceptional circum lance the amount of 0 ygen remaining in the confinedspace may be in ufficient to support lime, 0 that per ons caught in the space become a phyxiated. Burning hydrocarbon fuel are them elve extingui hed when the level of oxygen inks below orne 16 per cent, wherea human being can continue breathing in an atmosphere wi.th as little a 8-10 per cent oxygen, More fr quentlythe dimin! hed level. of oxygen re lilt in the production of carbon monoxide carbon particle (black moke) and other product of incomplete cornbu tion. Where the hydrocarbon fuel i extingui hed, toxic fumes of. for example. unburned
1.87
You might also like
- Canadian Warbirds of the Second World War - Fighters, Bombers and Patrol AircraftFrom EverandCanadian Warbirds of the Second World War - Fighters, Bombers and Patrol AircraftNo ratings yet
- B-29 “Double Trouble” Is “Mister Bee”: Radar Photography of and Bombing Japan During World War II My North Carolinian Father in the Crew of the "Lone B-29" Boeing Superfortress Bomber Flying the Longest Nonstop Combat Mission of World War IIFrom EverandB-29 “Double Trouble” Is “Mister Bee”: Radar Photography of and Bombing Japan During World War II My North Carolinian Father in the Crew of the "Lone B-29" Boeing Superfortress Bomber Flying the Longest Nonstop Combat Mission of World War IINo ratings yet
- Nightstalkers: The Wright Project and the 868th Bomb Squadron in World War IIFrom EverandNightstalkers: The Wright Project and the 868th Bomb Squadron in World War IINo ratings yet
- Operation Colossus: The First British Airborne Raid of World War IIFrom EverandOperation Colossus: The First British Airborne Raid of World War IINo ratings yet
- Naval Innovation for the 21st Century: The Office of Naval Research Since the End of the Cold WarFrom EverandNaval Innovation for the 21st Century: The Office of Naval Research Since the End of the Cold WarNo ratings yet
- British Warship Recognition: The Perkins Identification Albums: Volume II: Armoured Ships 1860-1895, Monitors and Aviation ShipsFrom EverandBritish Warship Recognition: The Perkins Identification Albums: Volume II: Armoured Ships 1860-1895, Monitors and Aviation ShipsRating: 5 out of 5 stars5/5 (2)
- Japanese Submarine Losses to Allied Submarines In World War 2From EverandJapanese Submarine Losses to Allied Submarines In World War 2No ratings yet
- Battleship Warspite: detailed in the original builders' plansFrom EverandBattleship Warspite: detailed in the original builders' plansNo ratings yet
- SuperFort, Vol.1, No.2, 25 Dec 1944Document7 pagesSuperFort, Vol.1, No.2, 25 Dec 1944JapanAirRaidsNo ratings yet
- United States Marine Corps Aviation Squadron Lineage, Insignia & HistoryFrom EverandUnited States Marine Corps Aviation Squadron Lineage, Insignia & HistoryNo ratings yet
- Engineer Aviation Units In The Southwest Pacific Theater During WWIIFrom EverandEngineer Aviation Units In The Southwest Pacific Theater During WWIINo ratings yet
- Mahan Goes To War: Effects Of World War I On The US Navy’s Force Structure And Operational PlanningFrom EverandMahan Goes To War: Effects Of World War I On The US Navy’s Force Structure And Operational PlanningNo ratings yet
- Gators of Neptune: Naval Amphibious Planning for the Normandy InvasionFrom EverandGators of Neptune: Naval Amphibious Planning for the Normandy InvasionRating: 4.5 out of 5 stars4.5/5 (5)
- The Royal Navy's Reserves in War & Peace, 1903–2003From EverandThe Royal Navy's Reserves in War & Peace, 1903–2003Rating: 4 out of 5 stars4/5 (1)
- War Diary May 1943 (All)Document45 pagesWar Diary May 1943 (All)Seaforth Webmaster100% (1)
- Japanese Carriers and Victory in the Pacific: The Yamamoto OptionFrom EverandJapanese Carriers and Victory in the Pacific: The Yamamoto OptionNo ratings yet
- Attack Transport; The Story Of The U.S.S. Doyen [Illustrated Edition]From EverandAttack Transport; The Story Of The U.S.S. Doyen [Illustrated Edition]No ratings yet
- The Patricia Lynn Project: Vietnam War, the Early Years of Air IntelligenceFrom EverandThe Patricia Lynn Project: Vietnam War, the Early Years of Air IntelligenceNo ratings yet
- Homeland Air Defense Operations Record - Japanese Monograph NoDocument95 pagesHomeland Air Defense Operations Record - Japanese Monograph NoJapanAirRaidsNo ratings yet
- Naval Combat Operations - Jul 1945Document31 pagesNaval Combat Operations - Jul 1945CAP History LibraryNo ratings yet
- 21st Bomber Command Tactical Mission Report 29Document65 pages21st Bomber Command Tactical Mission Report 29JapanAirRaids100% (1)
- Naval Combat Operations - Dec 1945Document23 pagesNaval Combat Operations - Dec 1945CAP History LibraryNo ratings yet
- From Auster to Apache: The History of 656 Squadron RAF/ACC 1942–2012From EverandFrom Auster to Apache: The History of 656 Squadron RAF/ACC 1942–2012No ratings yet
- The RAF's Cross-Channel Offensive: Circuses, Ramrods, Rhubarbs and Rodeos 1941-1942From EverandThe RAF's Cross-Channel Offensive: Circuses, Ramrods, Rhubarbs and Rodeos 1941-1942No ratings yet
- Air Intelligence Report, V1N19Document9 pagesAir Intelligence Report, V1N19JapanAirRaidsNo ratings yet
- USSBS Report 65, Employment of Forces Under The Southwest Pacific Command, OCRDocument34 pagesUSSBS Report 65, Employment of Forces Under The Southwest Pacific Command, OCRJapanAirRaidsNo ratings yet
- History of the 91st Aero Squadron Air Service U.S.A. (WWI Centenary Series)From EverandHistory of the 91st Aero Squadron Air Service U.S.A. (WWI Centenary Series)No ratings yet
- Naval Combat Operations - Jan 1945Document35 pagesNaval Combat Operations - Jan 1945CAP History LibraryNo ratings yet
- Submarine Warfare of To-day How the Submarine Menace was Met and Vanquished, With Descriptions of the Inventions and Devices Used, Fast Boats, Mystery ShipsFrom EverandSubmarine Warfare of To-day How the Submarine Menace was Met and Vanquished, With Descriptions of the Inventions and Devices Used, Fast Boats, Mystery ShipsNo ratings yet
- The Story Of The Lafayette Escadrille Told By Its CommanderFrom EverandThe Story Of The Lafayette Escadrille Told By Its CommanderRating: 4 out of 5 stars4/5 (1)
- XX Bomber Command, Tactical Mission Report, No 43, 10 March 1945Document65 pagesXX Bomber Command, Tactical Mission Report, No 43, 10 March 1945JapanAirRaids100% (1)
- Heroes Beneath the Waves: True Submarine Stories of the Twentieth CenturyFrom EverandHeroes Beneath the Waves: True Submarine Stories of the Twentieth CenturyRating: 3 out of 5 stars3/5 (1)
- The Littorio Class: Italy's Last and Largest Battleships 1937-1948From EverandThe Littorio Class: Italy's Last and Largest Battleships 1937-1948Rating: 4 out of 5 stars4/5 (5)
- USSBS Report 7, Field Report Covering Air Raid Protection and Allied Subjects, Kobe, Japan, OCRDocument72 pagesUSSBS Report 7, Field Report Covering Air Raid Protection and Allied Subjects, Kobe, Japan, OCRJapanAirRaidsNo ratings yet
- War Diary - August 1942Document154 pagesWar Diary - August 1942Seaforth WebmasterNo ratings yet
- Aircraft Carrier Victorious: Detailed in the Original Builders' PlansFrom EverandAircraft Carrier Victorious: Detailed in the Original Builders' PlansRating: 5 out of 5 stars5/5 (1)
- Impact, B-29 StrikesDocument16 pagesImpact, B-29 StrikesJapanAirRaidsNo ratings yet
- A Pathfinder's War: An Extraordinary Tale of Surviving Over 100 Bomber Operations Against All OddsFrom EverandA Pathfinder's War: An Extraordinary Tale of Surviving Over 100 Bomber Operations Against All OddsNo ratings yet
- Joey Jacobson's War: A Jewish-Canadian Airman in the Second World WarFrom EverandJoey Jacobson's War: A Jewish-Canadian Airman in the Second World WarNo ratings yet
- Naval Combat Operations - May 1945Document43 pagesNaval Combat Operations - May 1945CAP History LibraryNo ratings yet
- Field Artillery: Including Maps and PhotographsFrom EverandField Artillery: Including Maps and PhotographsNo ratings yet
- British Artillery During Operation CorporateFrom EverandBritish Artillery During Operation CorporateRating: 5 out of 5 stars5/5 (2)
- TSR2 Precision Attack to Tornado: Navigation and Weapon DeliveryFrom EverandTSR2 Precision Attack to Tornado: Navigation and Weapon DeliveryNo ratings yet
- Critical German Submarine Operations Versus Allied Convoys During March 1943: An Operational AnalysisFrom EverandCritical German Submarine Operations Versus Allied Convoys During March 1943: An Operational AnalysisNo ratings yet
- Naval Combat Operations - Jun 1945Document37 pagesNaval Combat Operations - Jun 1945CAP History LibraryNo ratings yet
- 21st Bomber Command Tactical Mission Report 271, 274, OcrDocument74 pages21st Bomber Command Tactical Mission Report 271, 274, OcrJapanAirRaids100% (1)
- USSBS Report 42, The Japanese Wartime Standard of LivingDocument62 pagesUSSBS Report 42, The Japanese Wartime Standard of LivingJapanAirRaidsNo ratings yet
- The Optics of Ruination - Towards An Archaeological Approach To The Photography of The Japan Air RaidsDocument26 pagesThe Optics of Ruination - Towards An Archaeological Approach To The Photography of The Japan Air RaidsJapanAirRaids100% (1)
- Henry Arnold Diaries IIDocument453 pagesHenry Arnold Diaries IICAP History LibraryNo ratings yet
- Mapping Armageddon - The Cartography of Ruin in Occupied Japan PDFDocument25 pagesMapping Armageddon - The Cartography of Ruin in Occupied Japan PDFJapanAirRaids100% (4)
- Yearbook, 949 Engineer Aviation Topographic Company, 1945Document21 pagesYearbook, 949 Engineer Aviation Topographic Company, 1945JapanAirRaids100% (1)
- The Optics of Ruination - Towards An Archaeological Approach To The Photography of The Japan Air RaidsDocument26 pagesThe Optics of Ruination - Towards An Archaeological Approach To The Photography of The Japan Air RaidsJapanAirRaids100% (1)
- Incendiary Mission Report, Tokyo, RG18.57B.45Document42 pagesIncendiary Mission Report, Tokyo, RG18.57B.45JapanAirRaids100% (1)
- Fire Warfare: Incendiaries and Flame ThrowersDocument87 pagesFire Warfare: Incendiaries and Flame ThrowersJapanAirRaids100% (1)
- 東京大空襲・戦災資料センター、政治経済研究所出版物Document24 pages東京大空襲・戦災資料センター、政治経済研究所出版物JapanAirRaidsNo ratings yet
- USSBS Report 71a, Air Campaigns of The Pacific WarDocument91 pagesUSSBS Report 71a, Air Campaigns of The Pacific WarJapanAirRaids100% (4)
- War Journal, Ninth Bombardment Group, U.S. Army Air Forces, 1945Document29 pagesWar Journal, Ninth Bombardment Group, U.S. Army Air Forces, 1945JapanAirRaids100% (4)
- Study of Incendiary Bombings For Employment by The United States Army Air Forces, 1 October 1944, NARA M1655, Roll40,1o.43Document96 pagesStudy of Incendiary Bombings For Employment by The United States Army Air Forces, 1 October 1944, NARA M1655, Roll40,1o.43JapanAirRaidsNo ratings yet
- USSBS Report 71, The Fifth Air Force in The War Against JapanDocument144 pagesUSSBS Report 71, The Fifth Air Force in The War Against JapanJapanAirRaids100% (1)
- The Pacific Problem, 1924Document27 pagesThe Pacific Problem, 1924JapanAirRaids100% (1)
- XXI Bomber Command, Tactical Mission Report 4Document49 pagesXXI Bomber Command, Tactical Mission Report 4JapanAirRaidsNo ratings yet
- USSBS Report 17, Nakajima Aircraft CompanyDocument128 pagesUSSBS Report 17, Nakajima Aircraft CompanyJapanAirRaids100% (3)
- Piercing The Fog Intelligence and Army Air Forces Operations in World War IIDocument516 pagesPiercing The Fog Intelligence and Army Air Forces Operations in World War IIBob AndrepontNo ratings yet
- USSBS Report 35, Underground Production of Japanese AircraftDocument50 pagesUSSBS Report 35, Underground Production of Japanese AircraftJapanAirRaids100% (3)
- USSBS Report 16, Mitsubishi Heavy IndustriesDocument219 pagesUSSBS Report 16, Mitsubishi Heavy IndustriesJapanAirRaids100% (1)
- USSBS Report 54, The War Against Japanese Transportation, 1941-45Document206 pagesUSSBS Report 54, The War Against Japanese Transportation, 1941-45JapanAirRaids100% (2)
- XXI Bomber Command, Tactical Mission Report 1Document47 pagesXXI Bomber Command, Tactical Mission Report 1JapanAirRaidsNo ratings yet
- XXI Bomber Command, Tactical Mission Report 3Document48 pagesXXI Bomber Command, Tactical Mission Report 3JapanAirRaids100% (1)
- WWII 73rd Bomb WingDocument56 pagesWWII 73rd Bomb WingCAP History LibraryNo ratings yet
- Resume, 20th Air Force MissionsDocument343 pagesResume, 20th Air Force MissionsJapanAirRaids100% (4)
- USSBS Report 75, The Allied Campaign Against RabaulDocument139 pagesUSSBS Report 75, The Allied Campaign Against RabaulJapanAirRaidsNo ratings yet
- America, Air Power, and The Pacific, 1928Document20 pagesAmerica, Air Power, and The Pacific, 1928JapanAirRaids100% (2)
- USSBS Report 80, Reports of Ships Bombardment Survey Party, Kamaishi AreaDocument116 pagesUSSBS Report 80, Reports of Ships Bombardment Survey Party, Kamaishi AreaJapanAirRaidsNo ratings yet
- USSBS Report 89, Effects of Surface Bombardments On Japanese War PotentialDocument45 pagesUSSBS Report 89, Effects of Surface Bombardments On Japanese War PotentialJapanAirRaidsNo ratings yet
- USSBS Report 73, Campaigns of The Pacific WarDocument423 pagesUSSBS Report 73, Campaigns of The Pacific WarJapanAirRaids100% (2)
- USSBS Report 76, The Allied Campaign Against WotjeDocument192 pagesUSSBS Report 76, The Allied Campaign Against WotjeJapanAirRaidsNo ratings yet
- USSBS Report 77, Reduction of TrukDocument19 pagesUSSBS Report 77, Reduction of TrukJapanAirRaids100% (1)










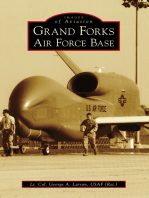





![Grand Fleet Days [Illustrated Edition]](https://imgv2-1-f.scribdassets.com/img/word_document/293581340/149x198/704a6e7ed7/1617234266?v=1)





![Attack Transport; The Story Of The U.S.S. Doyen [Illustrated Edition]](https://imgv2-1-f.scribdassets.com/img/word_document/293581022/149x198/89127cfc41/1627645394?v=1)