You might also like
- 1 s2.0 S1600613522146149 MainDocument14 pages1 s2.0 S1600613522146149 Mainomarcucho29No ratings yet
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- Vivra Tucson Study SheetsDocument58 pagesVivra Tucson Study SheetsRobert Davidson, M.D., Ph.D.No ratings yet
- Evidence Grading SystemDocument11 pagesEvidence Grading SystemCynthia Semá BaltazarNo ratings yet
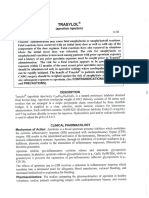
- Trasylol: (Aprotinin Injection)Document11 pagesTrasylol: (Aprotinin Injection)Ega MegawatiNo ratings yet
- ContentServer - Asp 2Document9 pagesContentServer - Asp 2witaparamitaNo ratings yet
- Telazol Ketaxyla in RatsDocument7 pagesTelazol Ketaxyla in RatsLab Diagklin FKH UBNo ratings yet
- Treatment With Am 80Document7 pagesTreatment With Am 80anisa rachmitaNo ratings yet
- Adipocytes Viability After Suction-Assisted Lipoplasty: Does The Technique Matter? HARATS, 2016 PDFDocument6 pagesAdipocytes Viability After Suction-Assisted Lipoplasty: Does The Technique Matter? HARATS, 2016 PDFCristhian DíazNo ratings yet
- 406 - Respiratory Therapy Consult Service HandbookDocument28 pages406 - Respiratory Therapy Consult Service HandbookIkhsan JohnsonNo ratings yet
- Long-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyDocument22 pagesLong-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyFlore HountondjiNo ratings yet
- HOI160023supp1 Prod PDFDocument10 pagesHOI160023supp1 Prod PDFcassieNo ratings yet
- Extubación TemDocument7 pagesExtubación TemMelina AlcaineNo ratings yet
- Duration of Adjuvant Oxaliplatin-Based Therapy For Stage III Colon Cancer - The ASCO PostDocument1 pageDuration of Adjuvant Oxaliplatin-Based Therapy For Stage III Colon Cancer - The ASCO PostNikos PapaioannouNo ratings yet
- JB&PHDocument6 pagesJB&PHjbenitesvilchezNo ratings yet
- Artificial HeartDocument47 pagesArtificial HeartAlaa EmadNo ratings yet
- QUIMIOEMBO + SORAFENIB TACTIS Trial 2019Document10 pagesQUIMIOEMBO + SORAFENIB TACTIS Trial 2019osrinconNo ratings yet
- ATLS 10th Edition Update Summary - Banana Bag Blog - Emergency Medicine BlogDocument21 pagesATLS 10th Edition Update Summary - Banana Bag Blog - Emergency Medicine BlogapisaraearthNo ratings yet
- Tenecteplase To Replace Alteplase Comparing ThromDocument2 pagesTenecteplase To Replace Alteplase Comparing ThromAlex DegraciaNo ratings yet
- 2017 EACTS/EACTA Guidelines On Patient Blood Management For Adult Cardiac SurgeryDocument33 pages2017 EACTS/EACTA Guidelines On Patient Blood Management For Adult Cardiac SurgeryBea AnabellaNo ratings yet
- STELLARmanuscriptDocument17 pagesSTELLARmanuscriptperjadanutNo ratings yet
- Thrombolysis Beyond 4.5 H in Acute Ischemic StrokeDocument8 pagesThrombolysis Beyond 4.5 H in Acute Ischemic StrokeLUIS AYALANo ratings yet
- Blood 777722Document3 pagesBlood 777722liadiafaridaNo ratings yet
- Cisatracurium in Different Doses Versus AtracuriumSaudiJAnaeshDocument7 pagesCisatracurium in Different Doses Versus AtracuriumSaudiJAnaeshAbo OmarNo ratings yet
- Endovascular Therapy For Ischemic Stroke With Perfusion-Imaging SelectionDocument10 pagesEndovascular Therapy For Ischemic Stroke With Perfusion-Imaging Selectioncitra dewiNo ratings yet
- 2023-Transfemoral Tricuspid Valve Replacement and One-Year Outcomes The TRISCEND StudyDocument12 pages2023-Transfemoral Tricuspid Valve Replacement and One-Year Outcomes The TRISCEND StudyNeison DuarteNo ratings yet
- Fita Fitrianti - EBCR Presentation - Comparison of Effectiveness and Survival Between TACE Versus TARE For Unresectable HCCDocument21 pagesFita Fitrianti - EBCR Presentation - Comparison of Effectiveness and Survival Between TACE Versus TARE For Unresectable HCCFita FitriantiNo ratings yet
- En Do Vascular Stenting or Carotid My For Treatment of Carotid Stenosis A Meta AnalysisDocument6 pagesEn Do Vascular Stenting or Carotid My For Treatment of Carotid Stenosis A Meta Analysisjohn_smith_532No ratings yet
- Esophagus Suprafirefly Plan ComparisonDocument7 pagesEsophagus Suprafirefly Plan Comparisonapi-396702708No ratings yet
- Cancer Lung Chemotherapy Regimen 3.4 March 2015Document69 pagesCancer Lung Chemotherapy Regimen 3.4 March 2015Jenny MárquezNo ratings yet
- Trastuzumab en Adyuvancia: Mr2 Sally Paredes Noguni Hnerm - Oncologia MedicaDocument20 pagesTrastuzumab en Adyuvancia: Mr2 Sally Paredes Noguni Hnerm - Oncologia MedicaSally Paredes NoguniNo ratings yet
- Trial: Tailorx: Trial Assigning Individualized Options For Treatment (RX)Document4 pagesTrial: Tailorx: Trial Assigning Individualized Options For Treatment (RX)Natalia QuinteroNo ratings yet
- Lung Cancer ManagementDocument126 pagesLung Cancer ManagementdjonesthoracicNo ratings yet
- Freeman 2008Document7 pagesFreeman 2008miguel pichiusaNo ratings yet
- Contrasting Time - and Rate-Based Approaches For The Assessment of Drug-Induced QT ChangesDocument10 pagesContrasting Time - and Rate-Based Approaches For The Assessment of Drug-Induced QT ChangesLuciana OliveiraNo ratings yet
- Tenecteplase For The Treatment of Acute Ischemic Stroke: A Review of Completed and Ongoing Randomized Controlled TrialsDocument8 pagesTenecteplase For The Treatment of Acute Ischemic Stroke: A Review of Completed and Ongoing Randomized Controlled TrialsyoggihermawanNo ratings yet
- Biology Project TheoryDocument16 pagesBiology Project TheoryAntra ashraNo ratings yet
- 10 1016@j Ejca 2019 10 025Document8 pages10 1016@j Ejca 2019 10 025habib diopNo ratings yet
- Sadamasa Ogasawara, MD, S. Ben Freedman,, David T. Kelly, MB, FaccDocument5 pagesSadamasa Ogasawara, MD, S. Ben Freedman,, David T. Kelly, MB, FaccArthur AlbertNo ratings yet
- If HP Cancer Guide br006 Adjuvant RT DcisDocument7 pagesIf HP Cancer Guide br006 Adjuvant RT Dcisrusgal8992No ratings yet
- Paracetamol: 1.1 Chemical and Physical DataDocument49 pagesParacetamol: 1.1 Chemical and Physical DataKimskiusNo ratings yet
- Acute Promyelocytic LeukemiaDocument46 pagesAcute Promyelocytic LeukemiaKartthik ShanmugamNo ratings yet
- Trasylol Ti: Administration. The Risk For A Fatal Reaction Appears To Be Greater Upon ReDocument15 pagesTrasylol Ti: Administration. The Risk For A Fatal Reaction Appears To Be Greater Upon ReNARESH JANDIALNo ratings yet
- Falstrom 1997Document6 pagesFalstrom 1997Igor DemićNo ratings yet
- The North American Vasovagal Pacemaker Study (VPS)Document5 pagesThe North American Vasovagal Pacemaker Study (VPS)Kat ZNo ratings yet
- Ejhf 81Document7 pagesEjhf 81Heather PorterNo ratings yet
- Current Therapeutic ResearchDocument6 pagesCurrent Therapeutic ResearchVincent ReyesNo ratings yet
- CMDA Regurgitation Vomiting and AspirationDocument5 pagesCMDA Regurgitation Vomiting and AspirationJavier Fernando Cabezas MeloNo ratings yet
- Body Weight (G) CBV (ML) 1% (ML) 10% (ML)Document5 pagesBody Weight (G) CBV (ML) 1% (ML) 10% (ML)Rooney RoyNo ratings yet
- Thesis Topics For MD PharmacologyDocument6 pagesThesis Topics For MD Pharmacologykatyallenrochester100% (1)
- Abstracts From The Global Embolization Sympo 2021 Journal of Vascular and inDocument21 pagesAbstracts From The Global Embolization Sympo 2021 Journal of Vascular and infreedy freedyNo ratings yet
- CardioRenal SyndromeDocument60 pagesCardioRenal Syndromeswaleh breik misfirNo ratings yet
- TAVI Vs CVA MetaanalisisDocument8 pagesTAVI Vs CVA Metaanalisiscar19No ratings yet
- Antiplatelet Therapy September 2013Document31 pagesAntiplatelet Therapy September 2013Randilufti SantosoNo ratings yet
- 17Document6 pages17Hedya Nadhrati SururaNo ratings yet
- Clinical and Translational Radiation Oncology: Original Research ArticleDocument6 pagesClinical and Translational Radiation Oncology: Original Research ArticleGörkem TürkkanNo ratings yet
- Predictores Exitosos en Destete de VentilaciónDocument25 pagesPredictores Exitosos en Destete de VentilaciónJesus PerezNo ratings yet
- Seb Ebm 16-17 PDFDocument100 pagesSeb Ebm 16-17 PDFWendy SitumorangNo ratings yet
- Persistent AFDocument16 pagesPersistent AFHafiz Wajid SadiqNo ratings yet
- Memorial Nursing School EssaysDocument4 pagesMemorial Nursing School EssaysSummer SeedsNo ratings yet
- My Pediatric Rotation ReflectionsDocument4 pagesMy Pediatric Rotation ReflectionsAdepoju Victor AbiolaNo ratings yet
- 1brisbane Final ReportDocument49 pages1brisbane Final ReportAustralian Human Rights100% (1)
- SRNA Orientation ChecklistDocument40 pagesSRNA Orientation Checklistihtisham1No ratings yet
- Project Green Apple V06Document7 pagesProject Green Apple V06Dudi KumarNo ratings yet
- Wenzhou People's HospitalDocument14 pagesWenzhou People's HospitalOmega SonnadaraNo ratings yet
- BCAS SoP For Screening of Passengers With Special Needs and Medical ConditionsDocument6 pagesBCAS SoP For Screening of Passengers With Special Needs and Medical ConditionsDisability Rights Alliance100% (2)
- Hospital Care in 2030Document2 pagesHospital Care in 2030Edgard SantosNo ratings yet
- Service Manual A100Document54 pagesService Manual A100erika50% (2)
- Case Clerking Hernia PDFDocument13 pagesCase Clerking Hernia PDFSoa ShahNo ratings yet
- Nursing Assessment in Family Nursing PracticeDocument2 pagesNursing Assessment in Family Nursing PracticeThrecia RotaNo ratings yet
- Phlebotomy Procedure 3rd PDFDocument4 pagesPhlebotomy Procedure 3rd PDFFranciska Gledy AmbaritaNo ratings yet
- Deborah Bowman, John Spicer, Rehana Iqbal-Informed Consent - A Primer For Clinical Practice-Cambridge University Press (2012)Document107 pagesDeborah Bowman, John Spicer, Rehana Iqbal-Informed Consent - A Primer For Clinical Practice-Cambridge University Press (2012)Meliani R'KyMeyNo ratings yet
- Why OvercrowdedDocument44 pagesWhy Overcrowdedfv2010fvNo ratings yet
- Spirit Care Hospital & ClinicDocument14 pagesSpirit Care Hospital & ClinicSALIL SHANKARNo ratings yet
- Nurses' Knowledge Regarding Hand Hygiene and Its Individual and Organizational PredictorsDocument9 pagesNurses' Knowledge Regarding Hand Hygiene and Its Individual and Organizational PredictorsMastifa HanasitaNo ratings yet
- Article 2Document24 pagesArticle 2GelanWelaboNo ratings yet
- Three Components of Hospice Care PrintableDocument4 pagesThree Components of Hospice Care PrintableVette Angelikka Dela CruzNo ratings yet
- (Hamilton, 2003) The Four Levels of Evidence-Based PracticeDocument7 pages(Hamilton, 2003) The Four Levels of Evidence-Based PracticeZackNo ratings yet
- ASA Physical Status Classification System 2019Document2 pagesASA Physical Status Classification System 2019hquinarNo ratings yet
- ResumeDocument2 pagesResumeapi-347141638No ratings yet
- BPOC in Medicina PrimaraDocument3 pagesBPOC in Medicina PrimaraAlina GheNo ratings yet
- q5 Nursery SchoolDocument4 pagesq5 Nursery SchoolPK CheahNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument4 pagesInternational Journal of Pediatric Otorhinolaryngologyzaenal abidinNo ratings yet
- Hip FractureDocument1 pageHip FractureHAILIE23100% (3)
- Lsat PT 3Document36 pagesLsat PT 3scribdfree4mo100% (5)
- Ornap 37th Acsm FlyerDocument2 pagesOrnap 37th Acsm FlyerMj AndayogNo ratings yet
- Quality Assurance in NursingDocument17 pagesQuality Assurance in NursingSathish Rajamani88% (17)
- Frozen Shoulder SummaryDocument8 pagesFrozen Shoulder SummaryBobNo ratings yet
- Newborn Myelomeningocele Protocol PCMCDocument4 pagesNewborn Myelomeningocele Protocol PCMC77nurseynurseNo ratings yet