You might also like
- Allergy, Immunity and Tolerance in Early Childhood: The First Steps of the Atopic MarchFrom EverandAllergy, Immunity and Tolerance in Early Childhood: The First Steps of the Atopic MarchHans Ulrich WahnRating: 3 out of 5 stars3/5 (1)
- Vaccine IngredientsDocument4 pagesVaccine IngredientsK. Banteilang NonglangNo ratings yet
- Swine Flu Vaccine FactsheetDocument4 pagesSwine Flu Vaccine Factsheetmuzaffaruz5932No ratings yet
- VACCINESDocument8 pagesVACCINESzilikajainNo ratings yet
- ConcernIngredientsAnimalIMAC200906V02Final PDFDocument2 pagesConcernIngredientsAnimalIMAC200906V02Final PDFFarhan Ullah KhanNo ratings yet
- CDC - Workshop On Thimerosal in Vaccines - 1999Document5 pagesCDC - Workshop On Thimerosal in Vaccines - 1999Eric UramNo ratings yet
- Journal of Dairy Science Volume Issue 2017 (Doi 10.3168 - jds.2017-12660) Kaczorek, E. Małaczewska, J. Wójcik, R. Rękawek, W. Siwic - Phenotypic and Genotypic Antimicrobial Susceptibility PatternDocument12 pagesJournal of Dairy Science Volume Issue 2017 (Doi 10.3168 - jds.2017-12660) Kaczorek, E. Małaczewska, J. Wójcik, R. Rękawek, W. Siwic - Phenotypic and Genotypic Antimicrobial Susceptibility Patternyudi poponNo ratings yet
- Schwalfenberg Et Al, 2018 (AJI 1)Document6 pagesSchwalfenberg Et Al, 2018 (AJI 1)Artika Muliany TindaonNo ratings yet
- Antibiotic GuidelinesDocument38 pagesAntibiotic GuidelinesKomang Adhi AmertajayaNo ratings yet
- Overdosed Babies:: Are Multiple Vaccines Safe?Document0 pagesOverdosed Babies:: Are Multiple Vaccines Safe?AprianaRohman100% (1)
- Evidence That Food Proteins in Vaccines Cause The Development of Food Allergies and Its Implications For Vaccine Policy 2329 6631 1000137Document3 pagesEvidence That Food Proteins in Vaccines Cause The Development of Food Allergies and Its Implications For Vaccine Policy 2329 6631 1000137Engkiong GoNo ratings yet
- Faq Vaccines ImmunisationDocument18 pagesFaq Vaccines ImmunisationAngela MitchelleNo ratings yet
- Project Brief Malawi WebDocument8 pagesProject Brief Malawi Websergio alvesNo ratings yet
- Parasite Control in Pasture-Grazed Dairy Cattle: Are We at The Edge of A Precipice?Document7 pagesParasite Control in Pasture-Grazed Dairy Cattle: Are We at The Edge of A Precipice?Oktrestu Dwi PutraNo ratings yet
- Defining Outcomes: HE Ournal of EdiatricsDocument2 pagesDefining Outcomes: HE Ournal of EdiatricsRizki Nur AmaliaNo ratings yet
- Public-Health Risks of Melamine in Milk Products: The Printed Journal Includes An Image Merely For IllustrationDocument2 pagesPublic-Health Risks of Melamine in Milk Products: The Printed Journal Includes An Image Merely For IllustrationLuiza Nicoleta MoglanNo ratings yet
- Peds 2010-0309 FullDocument11 pagesPeds 2010-0309 FullIkmah FauzanNo ratings yet
- Notes: Vaccines, Abortion, & Fetal TissueDocument5 pagesNotes: Vaccines, Abortion, & Fetal Tissuejdm81No ratings yet
- Final D Vaccines White Paper1Document7 pagesFinal D Vaccines White Paper1mariandNo ratings yet
- BTE722 - 2aDocument65 pagesBTE722 - 2aRakesh bhukyaNo ratings yet
- Proceedings of The 16th Italian Association of Equine Veterinarians CongressDocument10 pagesProceedings of The 16th Italian Association of Equine Veterinarians CongressCabinet VeterinarNo ratings yet
- AMR Profiles of Common Mastitis Pathogens On Canadian Dairy FarmsDocument14 pagesAMR Profiles of Common Mastitis Pathogens On Canadian Dairy FarmsApril LarasatiNo ratings yet
- Panchaud Et Al-2012-The Journal of Clinical Pharmacology-MinDocument9 pagesPanchaud Et Al-2012-The Journal of Clinical Pharmacology-MinAnna NutsubidzeNo ratings yet
- Pharmacy Daily For Tue 25 Mar 2014 - UK NIP Approves Bexsero, Mental Health Study, New Bleeding App, Letter To The Editor and Much MoreDocument3 pagesPharmacy Daily For Tue 25 Mar 2014 - UK NIP Approves Bexsero, Mental Health Study, New Bleeding App, Letter To The Editor and Much MorepharmacydailyNo ratings yet
- Ryeqo Epar Risk Management Plan Summary - enDocument5 pagesRyeqo Epar Risk Management Plan Summary - enUmaima faizNo ratings yet
- ThimerosalDocument73 pagesThimerosalBruno ReyesNo ratings yet
- Farmacología AntimastiticosDocument30 pagesFarmacología AntimastiticosAndres Alejandro CoralNo ratings yet
- Verizon Ebook Q3 3 Pediatric ToxicologyDocument9 pagesVerizon Ebook Q3 3 Pediatric ToxicologycesarNo ratings yet
- The Time of COVID - Phillip AltmanDocument107 pagesThe Time of COVID - Phillip AltmanYunSang ShinNo ratings yet
- Preventive Veterinary Medicine: E. Rollin, K.C. Dhuyvetter, M.W. OvertonDocument8 pagesPreventive Veterinary Medicine: E. Rollin, K.C. Dhuyvetter, M.W. OvertonBharathidhasan SelvarasuNo ratings yet
- Vaccine Friendly PlanDocument4 pagesVaccine Friendly PlanAna Sampaio89% (9)
- The Informative Value of An Overview On Antibiotic Consumption, Treatment Efficacy and Cost of Clinical Mastitis at Farm LevelDocument8 pagesThe Informative Value of An Overview On Antibiotic Consumption, Treatment Efficacy and Cost of Clinical Mastitis at Farm LeveljsolvarelaNo ratings yet
- 98 Aflatoxin Reduction in Milk and Milk Products PDFDocument35 pages98 Aflatoxin Reduction in Milk and Milk Products PDFTaj 825No ratings yet
- AddddDocument14 pagesAddddapi-547718836No ratings yet
- Monkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowDocument7 pagesMonkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowariniNo ratings yet
- Cost-Benefit Paratuberculosis: Analysis Vaccination Against Dairy CattleDocument5 pagesCost-Benefit Paratuberculosis: Analysis Vaccination Against Dairy CattlearavaNo ratings yet
- Austprescr 44 119Document5 pagesAustprescr 44 119Ingook SongNo ratings yet
- Vaccine Ingredients: What You Should KnowDocument2 pagesVaccine Ingredients: What You Should KnowKomsos - AG et al.No ratings yet
- Vaccination: Dairy Hub Training Booklets TitlesDocument8 pagesVaccination: Dairy Hub Training Booklets TitlesQais KaisraniNo ratings yet
- Vaccine Components Fact SheetDocument5 pagesVaccine Components Fact Sheetachuthasaran@11No ratings yet
- 57 - Adverse Drug Reactions in Breastfed Less Than ImaginedDocument16 pages57 - Adverse Drug Reactions in Breastfed Less Than ImaginedsasNo ratings yet
- Masitis Bovina Control Basado en Medicina PreventivaDocument4 pagesMasitis Bovina Control Basado en Medicina PreventivaDaniela BuenoNo ratings yet
- Postpartum Dysgalactia in SowsDocument4 pagesPostpartum Dysgalactia in SowsJuanita JordanNo ratings yet
- Edible Vaccines: Promises and Challenges: Vrinda M Kurup Jaya ThomasDocument12 pagesEdible Vaccines: Promises and Challenges: Vrinda M Kurup Jaya ThomasBelaNo ratings yet
- Current Treatment Aspects of Bovine Reproductive DisordersDocument10 pagesCurrent Treatment Aspects of Bovine Reproductive DisordersTatiana LageNo ratings yet
- Vesterlund Et Al, 2007 - Safety Assessment of Lactobacillus Strains PDFDocument7 pagesVesterlund Et Al, 2007 - Safety Assessment of Lactobacillus Strains PDFDanilo SilvaNo ratings yet
- Pharmatutor: Edible Vaccine - A Great Boon in Medicinal ScienceDocument4 pagesPharmatutor: Edible Vaccine - A Great Boon in Medicinal ScienceShailendra YadavNo ratings yet
- Vaccines and Population ControlDocument113 pagesVaccines and Population Controltheuselesseater100% (9)
- Nutfruit March 2016 IvarssonDocument3 pagesNutfruit March 2016 IvarssonFred EricNo ratings yet
- Annex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleDocument175 pagesAnnex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleEfendi AnuarNo ratings yet
- Cat HerniasDocument4 pagesCat HerniasbogdanotiNo ratings yet
- Vaccine Plan: The Dr. Paul ApprovedDocument9 pagesVaccine Plan: The Dr. Paul Approvedpaul popescu100% (1)
- Antibiotic Growth-Promoters in Food Animals: Peter HughesDocument25 pagesAntibiotic Growth-Promoters in Food Animals: Peter Hughesmekyno32No ratings yet
- A44 CMAJ Reducing The Pain of Childhood VaccinationDocument7 pagesA44 CMAJ Reducing The Pain of Childhood VaccinationGabriel CampolinaNo ratings yet
- Main Challenges in Poultry Farming: Hatchery Vaccination: Mohamed Faizal Abdul-CareemDocument25 pagesMain Challenges in Poultry Farming: Hatchery Vaccination: Mohamed Faizal Abdul-CareemN SipyonNo ratings yet
- ProceedingsDocument28 pagesProceedingsdjordjevetNo ratings yet
- Antiinfective Properties of Human MilkDocument6 pagesAntiinfective Properties of Human Milkkiko arrojasNo ratings yet
- Antiallergic Effects of ProbioticsDocument4 pagesAntiallergic Effects of ProbioticsputrinaraheswariNo ratings yet
- BIMA Oxford AZ Vaccine Detailed Position StatementDocument5 pagesBIMA Oxford AZ Vaccine Detailed Position StatementVegha NedyaNo ratings yet
- Probiotics and Preterm Infants A Position Paper.26 ShareDocument17 pagesProbiotics and Preterm Infants A Position Paper.26 Shareendy tovarNo ratings yet
- Histopathology Easy Mnemonic by ShahDocument18 pagesHistopathology Easy Mnemonic by ShahShah MohammedNo ratings yet
- Quick Quiz: Number of Yeast CellsDocument2 pagesQuick Quiz: Number of Yeast CellsVictor Barber SanchisNo ratings yet
- NCHSE Infection Control TESTDocument4 pagesNCHSE Infection Control TESTnurse1990No ratings yet
- Bio ProjectDocument25 pagesBio Projectlipi galotNo ratings yet
- ShingrixDocument6 pagesShingrixMarcus YoonNo ratings yet
- Portfolio IN Community Health Nursing: Submitted byDocument7 pagesPortfolio IN Community Health Nursing: Submitted byJay VillasotoNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination Detailsbd sinarbarakahNo ratings yet
- Indonesia National Immunization Program:: Dr. Prima Yosephine Epi Manager Moh IndonesiaDocument19 pagesIndonesia National Immunization Program:: Dr. Prima Yosephine Epi Manager Moh IndonesiaAstri KhairanaNo ratings yet
- 27 Best Coverage of Government - Suzy Davis - Katelyn Mary SkaggsDocument11 pages27 Best Coverage of Government - Suzy Davis - Katelyn Mary SkaggsSteve TaylorNo ratings yet
- The President Cory Aquino-HealthDocument4 pagesThe President Cory Aquino-HealthJesiah PascualNo ratings yet
- Thesis On Respiratory SystemDocument96 pagesThesis On Respiratory SystemDr Nimit ShahNo ratings yet
- Genomics BLAST AssignmentDocument12 pagesGenomics BLAST AssignmentDaniel Suarez100% (1)
- UICC Annual Report 2008Document48 pagesUICC Annual Report 2008schreamonn5515No ratings yet
- MRNA Vaccine Against Avian FluDocument5 pagesMRNA Vaccine Against Avian Fluanjum_niaziNo ratings yet
- Fernando - Sico - Elo - (181111010) Bahasa InggrisDocument2 pagesFernando - Sico - Elo - (181111010) Bahasa InggrisAsicoNo ratings yet
- Vaccines and Related Biological Products Advisory Committee MeetingDocument64 pagesVaccines and Related Biological Products Advisory Committee MeetingJim HoftNo ratings yet
- Brgy. Tonsuya Morbidity Week 36Document56 pagesBrgy. Tonsuya Morbidity Week 36Kathy OrtizNo ratings yet
- Social Exclusion Caste Health - A Review Based On The SocialDocument9 pagesSocial Exclusion Caste Health - A Review Based On The SocialSanthosh TekumalNo ratings yet
- Part III Final CDX 2bDocument15 pagesPart III Final CDX 2bBethrice MelegritoNo ratings yet
- TrepDocument50 pagesTrepMiguel Adrian GaonaNo ratings yet
- Sentimental Medicine PDFDocument8 pagesSentimental Medicine PDF杨飞燕No ratings yet
- RX Guide Delivering GoodsDocument9 pagesRX Guide Delivering GoodsjesakuNo ratings yet
- Other: RegionDocument4 pagesOther: RegionJoseph RepotenteNo ratings yet
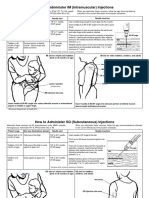
- Im SQ Admin PDFDocument2 pagesIm SQ Admin PDFAlvin JjNo ratings yet
- Prioritization of Mabs During Resource Shortages 20211229Document3 pagesPrioritization of Mabs During Resource Shortages 20211229News10NBCNo ratings yet
- Aerobic Non-Spore Forming Gram-Positive BacilliDocument31 pagesAerobic Non-Spore Forming Gram-Positive BacilliCagar Irwin TaufanNo ratings yet
- Late Shri Vinod Kumar MittalDocument6 pagesLate Shri Vinod Kumar MittaldasohamathNo ratings yet
- My Fiel Report 2018Document24 pagesMy Fiel Report 2018Popyeninawa HanyehaitilaNo ratings yet
- 2 Circle Venn Diagram 1Document1 page2 Circle Venn Diagram 1Mica RothenseeNo ratings yet
- Bacterial Sinusitis in Children: AcuteDocument11 pagesBacterial Sinusitis in Children: AcutefriscahalimNo ratings yet
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (6)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthFrom EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthRating: 4 out of 5 stars4/5 (7)
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthFrom EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNo ratings yet
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedNo ratings yet
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryFrom EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryRating: 4 out of 5 stars4/5 (6)
- Sickening: How Big Pharma Broke American Health Care and How We Can Repair ItFrom EverandSickening: How Big Pharma Broke American Health Care and How We Can Repair ItRating: 4 out of 5 stars4/5 (9)
- The Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeFrom EverandThe Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeRating: 3.5 out of 5 stars3.5/5 (7)
- The Inescapable Immune Escape PandemicFrom EverandThe Inescapable Immune Escape PandemicRating: 5 out of 5 stars5/5 (1)
- War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicFrom EverandWar on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicRating: 4 out of 5 stars4/5 (7)
- Microbiological Quality of FoodsFrom EverandMicrobiological Quality of FoodsL SlanetzNo ratings yet
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"From EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Rating: 3.5 out of 5 stars3.5/5 (3)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (15)
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadFrom EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadRating: 4.5 out of 5 stars4.5/5 (3)
- Epidemics and Society: From the Black Death to the PresentFrom EverandEpidemics and Society: From the Black Death to the PresentRating: 4.5 out of 5 stars4.5/5 (9)
- Arthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefFrom EverandArthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefNo ratings yet
- Make America Healthy Again: How Bad Behavior and Big Government Caused a Trillion-Dollar CrisisFrom EverandMake America Healthy Again: How Bad Behavior and Big Government Caused a Trillion-Dollar CrisisNo ratings yet
- The Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusFrom EverandThe Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusRating: 4.5 out of 5 stars4.5/5 (10)
- The Gut-loving Cookbook: Over 65 deliciously simple, gut-friendly recipes from The Gut StuffFrom EverandThe Gut-loving Cookbook: Over 65 deliciously simple, gut-friendly recipes from The Gut StuffNo ratings yet
- Panic Attack: Playing Politics with Science in the Fight Against COVID-19From EverandPanic Attack: Playing Politics with Science in the Fight Against COVID-19Rating: 4.5 out of 5 stars4.5/5 (10)