You might also like
- Guidelines For Pre Submission Seminar-LPUDocument1 pageGuidelines For Pre Submission Seminar-LPUsridharNo ratings yet
- Patterns of PNFDocument39 pagesPatterns of PNFsridhar100% (1)
- Lower Limb Evaluation Format Lower Limb Fracture Assesstment FormDocument12 pagesLower Limb Evaluation Format Lower Limb Fracture Assesstment FormsridharNo ratings yet
- Adverse Reaction To DrugsDocument22 pagesAdverse Reaction To DrugssridharNo ratings yet
- Nerve Conduction Velocity StudiesDocument12 pagesNerve Conduction Velocity StudiessridharNo ratings yet
- Ankle MobilizationDocument16 pagesAnkle MobilizationsridharNo ratings yet
- Brachial Plexus InjuryDocument43 pagesBrachial Plexus InjurysridharNo ratings yet
- 4 NCV1Document100 pages4 NCV1sridharNo ratings yet
- Imaging Findings and Clinical Correlation: Cerebral Herniation SyndromesDocument64 pagesImaging Findings and Clinical Correlation: Cerebral Herniation SyndromessridharNo ratings yet
- Tardieu ScaleDocument2 pagesTardieu ScalesridharNo ratings yet
- Vinayagar Agaval - Avvaiyar PDFDocument17 pagesVinayagar Agaval - Avvaiyar PDFkckejaman100% (1)
- Clavicle FractureDocument4 pagesClavicle FracturesridharNo ratings yet
- Tardieu ScaleDocument2 pagesTardieu ScalesridharNo ratings yet
- Brain Abscess PDFDocument28 pagesBrain Abscess PDFdoctordilafrozaNo ratings yet
- Geetha Mandir Bhawan, Model Town, PhagwaraDocument1 pageGeetha Mandir Bhawan, Model Town, PhagwarasridharNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Equipment MaintenanceDocument12 pagesEquipment MaintenanceGabriel OgbuNo ratings yet
- Punctuation Question 1: Click Me To See The Correct AnswerDocument5 pagesPunctuation Question 1: Click Me To See The Correct AnswerRakanNo ratings yet
- Adinda Tri Kurnia Putri - 2011313001 - A32020Document2 pagesAdinda Tri Kurnia Putri - 2011313001 - A32020allvi dayu nengsihNo ratings yet
- 2018 5-4 Care PlanningDocument4 pages2018 5-4 Care PlanningEd SchnurnbergerNo ratings yet
- Essentials of Medical Laboratory Practice Lieseke Constance L SRGDocument579 pagesEssentials of Medical Laboratory Practice Lieseke Constance L SRGAlexandr TrotskyNo ratings yet
- Atypical Parkinsonian Disorders PDFDocument515 pagesAtypical Parkinsonian Disorders PDFskyclad_21100% (3)
- Effectiveness of Neurofeedback Therapy FDocument5 pagesEffectiveness of Neurofeedback Therapy FLu CoelhoNo ratings yet
- Philo 3h NotesDocument5 pagesPhilo 3h Notesapi-3743951100% (3)
- Treatment of Gingival Recession by CoronallyDocument3 pagesTreatment of Gingival Recession by CoronallyIkhlasulAmalSangadjiNo ratings yet
- Masters ThesisDocument33 pagesMasters ThesisChristine Elaine Batusin IlaganNo ratings yet
- 3) Growth of Service SectorDocument9 pages3) Growth of Service SectorAMIN BUHARI ABDUL KHADER100% (1)
- Diver Medical - Physician S Evaluation FormDocument1 pageDiver Medical - Physician S Evaluation Formcrispin quadrosNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective: Short Term: IndependentDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective: Short Term: IndependentGuillao LensNo ratings yet
- 1 4929631937565294920Document986 pages1 4929631937565294920MAURICE022100% (2)
- Daily QuestionsDocument31 pagesDaily QuestionsVidisha ShekhawatNo ratings yet
- Tribhuvan University Teaching Hospital PDFDocument4 pagesTribhuvan University Teaching Hospital PDFashqNo ratings yet
- Contributions of Ibn Zuhr (Avenzoar) To The Progress of Medicine and UrologyDocument7 pagesContributions of Ibn Zuhr (Avenzoar) To The Progress of Medicine and UrologyRabie E. Abdel-HalimNo ratings yet
- Dental Practice ManagementDocument4 pagesDental Practice ManagementMahmoud MansourNo ratings yet
- Category B Emirates Insurance PDFDocument5 pagesCategory B Emirates Insurance PDFDonald HamiltonNo ratings yet
- Microsoft Word - DS03 - Paper - 1.1Document8 pagesMicrosoft Word - DS03 - Paper - 1.1kuridisanjeevNo ratings yet
- Extra Care Plus: Bajaj AllianzDocument18 pagesExtra Care Plus: Bajaj AllianzSushma SrivastavaNo ratings yet
- Case Study Dorothea Orem (Francar Jade For Sbmission) - TFNDocument2 pagesCase Study Dorothea Orem (Francar Jade For Sbmission) - TFNFrancar Jade De VeraNo ratings yet
- Conceptual Model of HRQoLDocument7 pagesConceptual Model of HRQoLNursyafiq Ali ShibramulisiNo ratings yet
- Our Fragmented Health Care SystemDocument4 pagesOur Fragmented Health Care Systemnchc-scribdNo ratings yet
- 366-Article Text-1258-1-10-20220824Document7 pages366-Article Text-1258-1-10-20220824YunitafazaksNo ratings yet
- Fridays LawsDocument2 pagesFridays LawsAHRMMNo ratings yet
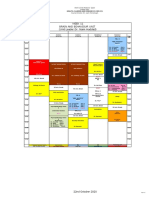
- Week 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)Document1 pageWeek 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)f3er3No ratings yet
- Teaching Plan Wound CareDocument3 pagesTeaching Plan Wound CareLody Lean CruzNo ratings yet
- Texas Suicide Prevention Council SymposiumDocument7 pagesTexas Suicide Prevention Council SymposiumShirley Pigott MDNo ratings yet
- Advantage and Disadvantage of BreastfeedingDocument2 pagesAdvantage and Disadvantage of BreastfeedingKathleen ColinioNo ratings yet