You might also like
- Monastery of The Seven Rays - Year 1Document193 pagesMonastery of The Seven Rays - Year 1Lykathea Harmony Pax100% (5)
- Embedded Images Non Verbal Reasoning Questions and AnswersDocument27 pagesEmbedded Images Non Verbal Reasoning Questions and AnswersAditya DeshmukhNo ratings yet
- Male GU ExamDocument5 pagesMale GU ExamOmar Farid ElgebalyNo ratings yet
- 1-Adrenocorticosteroids Chapter39Document94 pages1-Adrenocorticosteroids Chapter39hamidNo ratings yet
- Antipsychotic Drugs: Conventional AntipsychoticsDocument16 pagesAntipsychotic Drugs: Conventional AntipsychoticsApple MaeNo ratings yet
- Surgical Management:: Nursing CareDocument3 pagesSurgical Management:: Nursing CareVarsha Net CafeNo ratings yet
- Description: Congestive Heart FailureDocument22 pagesDescription: Congestive Heart FailurePinklet Arleena CubianNo ratings yet
- Chapter 19 Heart Marie BDocument29 pagesChapter 19 Heart Marie BomarNo ratings yet
- Case Study - Wal-Mart Failure in GermanyDocument5 pagesCase Study - Wal-Mart Failure in GermanyYasser SadekNo ratings yet
- Test Bank For Lehninger Principles of Biochemistry Sixth EditionDocument11 pagesTest Bank For Lehninger Principles of Biochemistry Sixth Editioncosimalocu68xb1No ratings yet
- NUR129 Endocrine Concept Mapping InstructorDocument8 pagesNUR129 Endocrine Concept Mapping InstructorAmber EssmanNo ratings yet
- Constipation: Stools ExplainedDocument4 pagesConstipation: Stools ExplainedArun MuralidharanNo ratings yet
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocument42 pagesHepatobiliary Disorders: Katrina Saludar Jimenez, R. NKatrinaJimenezNo ratings yet
- VolvulusDocument38 pagesVolvulusHector RaulNo ratings yet
- Gastrointestinal DrugsDocument45 pagesGastrointestinal DrugsCindy MaslagNo ratings yet
- Set 1Document62 pagesSet 1Alyssa MontimorNo ratings yet
- Enteral Feeding: Gastric Versus Post-Pyloric: Table 1Document22 pagesEnteral Feeding: Gastric Versus Post-Pyloric: Table 1tasmeow23No ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Dysrhythmias: Se Admin Anticoagulante, Cardioversion As PrescribedDocument10 pagesDysrhythmias: Se Admin Anticoagulante, Cardioversion As Prescribedyaneidys perezNo ratings yet
- FNP Final TestDocument10 pagesFNP Final TestNelson MandelaNo ratings yet
- Gastritis: Medical AffairDocument11 pagesGastritis: Medical AffairKomal KhanNo ratings yet
- Chapter 66 - ShockDocument9 pagesChapter 66 - ShockCrysta Venice Tapoc100% (1)
- Gastrointesti Nal Tract/Food PathwayDocument22 pagesGastrointesti Nal Tract/Food PathwayElpen FatrizalNo ratings yet
- Fluids and ElectrolytesDocument128 pagesFluids and Electrolytesmd6ztpydckNo ratings yet
- Ch. 1, Lesson 1: What Is The Next Gen NCLEXDocument4 pagesCh. 1, Lesson 1: What Is The Next Gen NCLEXChantelNo ratings yet
- AdultDocument295 pagesAdultKen WonNo ratings yet
- 4 Reading-PracticeDocument24 pages4 Reading-PracticeCườiLênNhéNo ratings yet
- Hyperemesis Gravidarum: Bleeding Complications of PregnancyDocument6 pagesHyperemesis Gravidarum: Bleeding Complications of PregnancykirbsNo ratings yet
- Hematologic System2Document70 pagesHematologic System2Jesus Mario LopezNo ratings yet
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- GI Notes For Exam 3Document4 pagesGI Notes For Exam 3cathyNo ratings yet
- Immunity 1Document6 pagesImmunity 1Tori RolandNo ratings yet
- Genitourinary Problem: Nephrotic Syndrome Wilm's Tumor ManagementDocument19 pagesGenitourinary Problem: Nephrotic Syndrome Wilm's Tumor ManagementJayson CruzNo ratings yet
- Hepatobiliary Disorders 2Document21 pagesHepatobiliary Disorders 2KatrinaJimenezNo ratings yet
- Week 11 - Ch. 36 - UrinaryDocument27 pagesWeek 11 - Ch. 36 - UrinaryMary SingletonNo ratings yet
- Medical Surgical Nursing - DiabetesDocument4 pagesMedical Surgical Nursing - Diabetestripj33100% (2)
- The Infant Should Always Be in A Rear-Facing Car Seat From Birth To 9.1 KGDocument7 pagesThe Infant Should Always Be in A Rear-Facing Car Seat From Birth To 9.1 KGSabhi Sandhu100% (1)
- ABC Dictionary of Urinary SystemDocument26 pagesABC Dictionary of Urinary Systemaby_romero9750% (2)
- Sinus Bradycardia: I. Sinus Dysrhythmias Description ManagementDocument4 pagesSinus Bradycardia: I. Sinus Dysrhythmias Description ManagementMargueretti Delos ReyesNo ratings yet
- Fundamental QuestionsDocument5 pagesFundamental QuestionsSheshe0% (3)
- Brain Dump NUR 213 FINALDocument37 pagesBrain Dump NUR 213 FINALkelsey jackson100% (1)
- CH 59 Care of Patients With Problems of The Biliary System and PancreasDocument28 pagesCH 59 Care of Patients With Problems of The Biliary System and Pancreasjrflores1284No ratings yet
- Nursing Management in Abdominal SurgeryDocument19 pagesNursing Management in Abdominal Surgeryejguy7777100% (2)
- VSim SARAH LIN For Nursing - Health Assessment POST QUIZDocument5 pagesVSim SARAH LIN For Nursing - Health Assessment POST QUIZWen RodsaNo ratings yet
- MS Final 46 Blood or Lymphatic DisorderDocument4 pagesMS Final 46 Blood or Lymphatic DisorderZachary T Hall0% (1)
- Jennifer Portillo Health Assessment VocabularyDocument9 pagesJennifer Portillo Health Assessment VocabularyJennifer PortilloNo ratings yet
- Acute Pancreatitis: J Koh & D ChengDocument7 pagesAcute Pancreatitis: J Koh & D ChengGloriaaaNo ratings yet
- MedSurg CH 44 & 45 Study GuideDocument5 pagesMedSurg CH 44 & 45 Study GuideMichele ShepardNo ratings yet
- Clinical Case Aki Presentation EportfolioDocument32 pagesClinical Case Aki Presentation Eportfolioapi-463444835No ratings yet
- Normocytic Anemia'sDocument14 pagesNormocytic Anemia'sbrown_chocolate87643No ratings yet
- Nclex (1301) (1) (1315)Document43 pagesNclex (1301) (1) (1315)Elizabeth SharmaNo ratings yet
- Colon CancerDocument7 pagesColon CancerKen Ancheta LagayadaNo ratings yet
- Shock and SIRSDocument85 pagesShock and SIRSBryan Mae H. DegorioNo ratings yet
- MedSurg GIDocument4 pagesMedSurg GIZachary T HallNo ratings yet
- RN GI Endoscopy, Operating RoomDocument4 pagesRN GI Endoscopy, Operating Roomapi-78554516100% (1)
- 2.hypertensive Disorders in PregnancyDocument8 pages2.hypertensive Disorders in PregnancyMuvenn KannanNo ratings yet
- GI NotesDocument19 pagesGI NotesBigBoostingNo ratings yet
- Tissue TransplantDocument20 pagesTissue TransplantEva Boje-JugadorNo ratings yet
- Adult Health III Final Study GuideDocument12 pagesAdult Health III Final Study GuideRyanne JNo ratings yet
- Review of Systems ANDREADocument7 pagesReview of Systems ANDREAAndrea Dora OrtalizNo ratings yet
- Cholesistitis (DR - Prema Hapsari, SPPD)Document28 pagesCholesistitis (DR - Prema Hapsari, SPPD)Niniek Iin F100% (1)
- Worksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Document3 pagesWorksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Emerald SpanglerNo ratings yet
- Clinical Case Study - Online Discussion Form Fall 2020-1Document14 pagesClinical Case Study - Online Discussion Form Fall 2020-1Sabrina Odies100% (1)
- Fetal Heart Rate Interpretation Adaptation To LaborDocument36 pagesFetal Heart Rate Interpretation Adaptation To Laboryolondanic100% (1)
- Nursing Pharmacology Drug Study GuideDocument15 pagesNursing Pharmacology Drug Study GuideChelsea SmithNo ratings yet
- E-News January 2013 PublicationDocument37 pagesE-News January 2013 PublicationGrand Lodge Free And Accepted Masons of FloridaNo ratings yet
- Module 2 Strategic ManagementDocument4 pagesModule 2 Strategic ManagementWalidahmad AlamNo ratings yet
- Pop Culture and The Rise of Social Media in The Philippines: An OverviewDocument2 pagesPop Culture and The Rise of Social Media in The Philippines: An OverviewDanielle MerlinNo ratings yet
- Potterton Performa System HE User GuideDocument12 pagesPotterton Performa System HE User GuideReUp2009No ratings yet
- New Customer Emails For Muhammad AliDocument17 pagesNew Customer Emails For Muhammad Aliknotship.comNo ratings yet
- Adaptation and Survival: of Organisms in The Changing WorldDocument3 pagesAdaptation and Survival: of Organisms in The Changing WorldAyka CantorNo ratings yet
- Lead Me Lord.Document1 pageLead Me Lord.jessie8165No ratings yet
- Folded Trie: Efficient Data Structure For All of UnicodeDocument21 pagesFolded Trie: Efficient Data Structure For All of Unicodeterminatory808No ratings yet
- General Active Directory Interview QuestionsDocument10 pagesGeneral Active Directory Interview Questionsbharath mylavarapuNo ratings yet
- Resume Pak AfandiDocument4 pagesResume Pak Afandimico wahyudiNo ratings yet
- Syllabus of Medical Licensing ExaminationDocument3 pagesSyllabus of Medical Licensing Examinationapi-370059967% (3)
- DUB01CB Eng PDFDocument4 pagesDUB01CB Eng PDFAnonymous hj273CMNo ratings yet
- PV Elite Training-MAWP Reduction PV EliteDocument8 pagesPV Elite Training-MAWP Reduction PV EliterakicbgNo ratings yet
- CPD Providers As of Feb 6, 2020Document733 pagesCPD Providers As of Feb 6, 2020John Mark ArcillaNo ratings yet
- Amateur PDFDocument218 pagesAmateur PDFAnonymous ToJLwXNo ratings yet
- CREDITOSDocument3 pagesCREDITOSJean RosaNo ratings yet
- Feasibility Study TemplateDocument21 pagesFeasibility Study TemplateRan Cyla TagleNo ratings yet
- Beza USA Finacial ReportDocument1 pageBeza USA Finacial ReportmikebezaconsultNo ratings yet
- UKMT - JMC - Junior Mathematical Challenge 2005 - QuestionsDocument10 pagesUKMT - JMC - Junior Mathematical Challenge 2005 - Questionsthatday826No ratings yet
- Pioneer VSX 417Document52 pagesPioneer VSX 417cristakeNo ratings yet
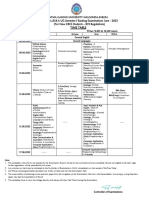
- UG Semesters I, II, & III Backlog Time-Table June-2023Document6 pagesUG Semesters I, II, & III Backlog Time-Table June-2023naganathNo ratings yet
- EI Install Manual GEN II 111418Document22 pagesEI Install Manual GEN II 111418mozhi selvamNo ratings yet
- LEEP System 1000 Directions For UseeDocument24 pagesLEEP System 1000 Directions For UseeFernando CosciaNo ratings yet
- Sli Ia 01Document3 pagesSli Ia 01Rose JessicaNo ratings yet
- Procedure Process For Glass Bottle ChandelierDocument4 pagesProcedure Process For Glass Bottle ChandelierKryzia Jelle CastillanoNo ratings yet