You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- FASD Brochure For Teachers: Aint MisbehavingDocument2 pagesFASD Brochure For Teachers: Aint Misbehavingfasdunited100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Self Concept QuestionnaireDocument5 pagesSelf Concept QuestionnaireNikeeta Singh100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ingles Primaria 3 PDFDocument6 pagesIngles Primaria 3 PDFJuan JugueraNo ratings yet
- ITC Lecture 1Document14 pagesITC Lecture 1hamzahanif91No ratings yet
- Children's Choirs KodalyDocument5 pagesChildren's Choirs KodalyTreyce BannermanNo ratings yet
- Rose Hinds ResumeDocument2 pagesRose Hinds Resumeapi-751527900No ratings yet
- CitesteDocument3 pagesCitesteCosmin MarianNo ratings yet
- Explainability and Interpretability For RetinopathyDocument2 pagesExplainability and Interpretability For RetinopathyAdem BRITAHNo ratings yet
- 4.3. Multilingualism (2022)Document37 pages4.3. Multilingualism (2022)carlesNo ratings yet
- Facilitating LearningsDocument2 pagesFacilitating LearningsMa Paula EncinaNo ratings yet
- Standard 3.2 - Plan, Structure and Sequence Learning ProgramsDocument3 pagesStandard 3.2 - Plan, Structure and Sequence Learning Programsapi-313880657No ratings yet
- Sammasati DSFDocument53 pagesSammasati DSFbharath_mv7No ratings yet
- file:///C:/Users/Asus/Downloads/334697616 Lesson 1 Human Cultural Variations Social Differences Social Change and Political Identities PDFDocument2 pagesfile:///C:/Users/Asus/Downloads/334697616 Lesson 1 Human Cultural Variations Social Differences Social Change and Political Identities PDFIgorota SheanneNo ratings yet
- AIDocument2 pagesAIAlexie AlmohallasNo ratings yet
- Rashid Ali CV ETIHADDocument2 pagesRashid Ali CV ETIHADmirahmedshahNo ratings yet
- 1605 CTP - Lesson Plan TemplateDocument5 pages1605 CTP - Lesson Plan TemplateAnna WangNo ratings yet
- Chapter 3Document52 pagesChapter 3MonahelmyNo ratings yet
- Introduction To Abnormal PsychologyDocument60 pagesIntroduction To Abnormal PsychologyNandini JagadeesanNo ratings yet
- DEVANSH's ResumeDocument1 pageDEVANSH's ResumeAman yadavNo ratings yet
- Alcohol ConsumptionDocument1 pageAlcohol Consumptionapi-550823265No ratings yet
- Project Progress Report ..2nd Year HND Electrical EngineeringDocument5 pagesProject Progress Report ..2nd Year HND Electrical EngineeringMullah FassudinNo ratings yet
- Daftar PustakaDocument5 pagesDaftar PustakaJuan SardiNo ratings yet
- Module 1. Lesson 2. Identifying Learners' Training RequirementsDocument9 pagesModule 1. Lesson 2. Identifying Learners' Training RequirementsGuenn SarmientoNo ratings yet
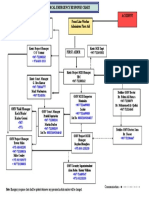
- Medical Emergency RESPONSE CHART - Doc - 1Document1 pageMedical Emergency RESPONSE CHART - Doc - 1Mohammed Ahmed NasherNo ratings yet
- Signed Off SMAW11 q1 m4 Fit-Up Welds Material v3Document33 pagesSigned Off SMAW11 q1 m4 Fit-Up Welds Material v3Christian Jake Respicio100% (1)
- Computer Science and Engineering. Complete UnitDocument7 pagesComputer Science and Engineering. Complete Unitmanuelpantoja79No ratings yet
- Narasimha ProjectDocument82 pagesNarasimha ProjectVamsi SakhamuriNo ratings yet
- Ficha-Ingl-4to. A-B - Semana 3Document3 pagesFicha-Ingl-4to. A-B - Semana 3wilder chiroqueNo ratings yet
- East Stroudsburg United Methodist Church: Welcome!Document6 pagesEast Stroudsburg United Methodist Church: Welcome!East Stroudsburg United Methodist ChurchNo ratings yet
- A Novel Approach For Churn Prediction Using Minimal Factor Selection ApproachDocument5 pagesA Novel Approach For Churn Prediction Using Minimal Factor Selection ApproachMalik GNo ratings yet