You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- PPG Lesson+4 States,+Nations,+and+GlobalizationDocument21 pagesPPG Lesson+4 States,+Nations,+and+GlobalizationKrishna DelacruzNo ratings yet
- Made, Not Born - Why Some Soldiers Are Better Than OthersDocument216 pagesMade, Not Born - Why Some Soldiers Are Better Than OthersHaning Tyas Cahya PratamaNo ratings yet
- Business Culture in British India PDFDocument17 pagesBusiness Culture in British India PDFshiv161No ratings yet
- Sel CVDocument2 pagesSel CVEfraim James Escamillas LantingNo ratings yet
- TalcottParsons - On The Concept of Power PDFDocument32 pagesTalcottParsons - On The Concept of Power PDFAna Cecilia MedinaNo ratings yet
- Open Letter To MS SwaminathanDocument9 pagesOpen Letter To MS SwaminathanEaswer SanNo ratings yet
- Croatia Trade Policy Regime Framework and ObjectivesDocument3 pagesCroatia Trade Policy Regime Framework and ObjectivesAna MariaNo ratings yet
- The Negative Effects of Free Trade Agreements On EmploymentDocument11 pagesThe Negative Effects of Free Trade Agreements On EmploymentRaymina CNo ratings yet
- Laws of Malaysia: Societies Act 1966Document69 pagesLaws of Malaysia: Societies Act 1966Anothai KumariNo ratings yet
- Revised Implementing Rules and Regulation (Ra 0163)Document30 pagesRevised Implementing Rules and Regulation (Ra 0163)Mica Joice FernandezNo ratings yet
- A Work of ArtificeDocument6 pagesA Work of Artificeriddhimashetty28No ratings yet
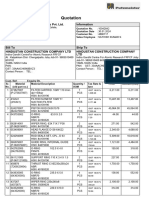
- Quotation: Putzmeister Concrete Machines Pvt. Ltd. InformationDocument4 pagesQuotation: Putzmeister Concrete Machines Pvt. Ltd. InformationsathishNo ratings yet
- Mesoamerican Studies Center ConferenceDocument8 pagesMesoamerican Studies Center ConferenceDifusión LAOMSNo ratings yet
- Sexual TextualDocument7 pagesSexual Textualcol890% (1)
- Excerpt From "Why I Am Not A Feminist" by Jessa Crispin.Document2 pagesExcerpt From "Why I Am Not A Feminist" by Jessa Crispin.OnPointRadio67% (3)
- Case SummaryDocument2 pagesCase SummaryAditya D TanwarNo ratings yet
- HAL SC ST CertificateDocument2 pagesHAL SC ST CertificateRuthvik ReddyNo ratings yet
- Private International Law and Its SourcesDocument77 pagesPrivate International Law and Its SourcesMike100% (1)
- Yes ProgrammeDocument2 pagesYes ProgrammeKenny LeeNo ratings yet
- Constitutional Law I: in Re Ching, Bar Matter No. 914Document2 pagesConstitutional Law I: in Re Ching, Bar Matter No. 914Bayani KamporedondoNo ratings yet
- Analysis - Arakan Army - A Powerful New Threat To The TatmadawDocument11 pagesAnalysis - Arakan Army - A Powerful New Threat To The TatmadawIndobhasa MogNo ratings yet
- Aijaz Ahmad - Aditya Bahl, Border-Crosser - SidecarDocument8 pagesAijaz Ahmad - Aditya Bahl, Border-Crosser - SidecarLeandro de Oliveira GalastriNo ratings yet
- English For Lawyers IIDocument138 pagesEnglish For Lawyers IIInggrid S. Bawias100% (1)
- Michael Cohen Letter To CongressDocument16 pagesMichael Cohen Letter To CongressRawStoryNo ratings yet
- 5.4.4 Practice - Intergroup Conflict (Practice)Document2 pages5.4.4 Practice - Intergroup Conflict (Practice)MarcelineNo ratings yet
- 4th Module 1Document18 pages4th Module 1Mha RizNo ratings yet
- English Proficiency LocalDocument3 pagesEnglish Proficiency LocalYvanne Kris IVNo ratings yet
- Local OrdinancesDocument14 pagesLocal OrdinancesAlmer Tanudra Vineyard ConstructionNo ratings yet
- Constitution Law Project On Misuse of Article 356Document14 pagesConstitution Law Project On Misuse of Article 356Thakur Prashant SinghNo ratings yet
- Pandi, BulacanDocument2 pagesPandi, BulacanSunStar Philippine NewsNo ratings yet