You might also like
- Ana Gašparović: Mentor: A. Žmegač HorvatDocument10 pagesAna Gašparović: Mentor: A. Žmegač HorvatDivine IncilloNo ratings yet
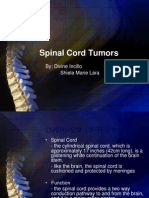
- Spinal Cord Tumors: By: Divine Incillo Shiela Marie LaraDocument27 pagesSpinal Cord Tumors: By: Divine Incillo Shiela Marie LaraDivine IncilloNo ratings yet
- RabiesDocument22 pagesRabiesDivine IncilloNo ratings yet
- Honors Physics - Work and EnergyDocument20 pagesHonors Physics - Work and EnergyDivine IncilloNo ratings yet
- Characteristics of Stool 869Document10 pagesCharacteristics of Stool 869Divine IncilloNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Serotonin PDFDocument4 pagesSerotonin PDFakghassan863No ratings yet
- Accessory Air Breathing OrgansDocument26 pagesAccessory Air Breathing Organskaushik mallickNo ratings yet
- 91-Article Text-150-1-10-20181022Document9 pages91-Article Text-150-1-10-20181022Sandy Wahyu DNo ratings yet
- MODULE 1 - Why Is Nutrition ImportantDocument6 pagesMODULE 1 - Why Is Nutrition ImportantDonna MarieNo ratings yet
- Parasitic Adaptation PDFDocument6 pagesParasitic Adaptation PDFmubarik Hayat50% (2)
- Digestive Care Package AdvancedDocument22 pagesDigestive Care Package AdvancedWwNo ratings yet
- Soiled Pants Pamphlet 2Document2 pagesSoiled Pants Pamphlet 2Sebastian OrtizNo ratings yet
- Histology of Digestive SystemDocument39 pagesHistology of Digestive Systemirakozehugue14No ratings yet
- Digestive System Anatomy and Physiology - NurseslabsDocument33 pagesDigestive System Anatomy and Physiology - NurseslabsMari FeNo ratings yet
- Ntestinal Intraepithelial LymphocytesDocument21 pagesNtestinal Intraepithelial LymphocytesEDGAR FUENMAYOR PIRELANo ratings yet
- Clisma - BastiDocument5 pagesClisma - BastiSese SekoNo ratings yet
- (1892) Fashion SlavesDocument48 pages(1892) Fashion SlavesHerbert Hillary Booker 2nd100% (2)
- Yanzlee P. Ananayo Grade 4-Bl. Sandor Science 4 Laboratory Activity #2 How Is Different Food Digested?Document3 pagesYanzlee P. Ananayo Grade 4-Bl. Sandor Science 4 Laboratory Activity #2 How Is Different Food Digested?Marvin SalvadorNo ratings yet
- Intestinal Obstruction2Document26 pagesIntestinal Obstruction2TwinkleNo ratings yet
- Digestion, Absorption, and MetabolismDocument6 pagesDigestion, Absorption, and MetabolismbananakyuNo ratings yet
- Intestinal AnastomosisDocument12 pagesIntestinal Anastomosisjosephgunter100% (6)
- The Human Intestinal Microbiome in Health and Disease: Review ArticleDocument11 pagesThe Human Intestinal Microbiome in Health and Disease: Review Articlepermen_lollypopzNo ratings yet
- Chapter 2Document64 pagesChapter 2elbannanNo ratings yet
- G8 Summative 1 Perf Task 1Document1 pageG8 Summative 1 Perf Task 1nicodemus balasuelaNo ratings yet
- Neet PG 2023 Imp TopicsDocument21 pagesNeet PG 2023 Imp TopicsAslesh AnandNo ratings yet
- Morbid Obesity Case StudyDocument12 pagesMorbid Obesity Case Studyapi-437064053No ratings yet
- Physiology of DigestionDocument15 pagesPhysiology of Digestionreema amynNo ratings yet
- Chapter 11-Human Body SystemDocument48 pagesChapter 11-Human Body SystemTrần MạnhNo ratings yet
- Product Catalogue 2010Document112 pagesProduct Catalogue 2010Dennis NguyenNo ratings yet
- Heterotrophic Nutrition PDFDocument10 pagesHeterotrophic Nutrition PDFNakshatra PaliwalNo ratings yet
- Anatomy and Physiology Digestive System - Ingests Food (Takes It In), Digests It (Breaks It Down) Into Nutrient Molecules, Absorbs TheDocument6 pagesAnatomy and Physiology Digestive System - Ingests Food (Takes It In), Digests It (Breaks It Down) Into Nutrient Molecules, Absorbs TheMark Nel NuñezNo ratings yet
- Products InformationDocument48 pagesProducts InformationRajat TripathiNo ratings yet
- IcdDocument30 pagesIcdSuryaAtmajayaNo ratings yet
- Injoere v2n2p46 enDocument33 pagesInjoere v2n2p46 enAndia BalabanNo ratings yet
- Surprises From Celiac Disease Scientific American August 2009Document8 pagesSurprises From Celiac Disease Scientific American August 2009Mihaly KovacsNo ratings yet