You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- NCM 112 N LECTURE MidtermDocument42 pagesNCM 112 N LECTURE MidtermVivien IgnacioNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medicine Clinics Guide: Summary of Bates Tables From DR DominguezDocument226 pagesMedicine Clinics Guide: Summary of Bates Tables From DR DominguezSaf DicamNo ratings yet
- Preoperative and Postoperative Care SeminarDocument50 pagesPreoperative and Postoperative Care SeminarRenuka Sivaram88% (8)
- 1) Introtuction To Emergency Medical CareDocument19 pages1) Introtuction To Emergency Medical CareRodrigo López Gutiérrez0% (1)
- Chapter 02Document69 pagesChapter 02api-3743202No ratings yet
- Chapter 04Document52 pagesChapter 04api-3743202No ratings yet
- Chapter 05Document43 pagesChapter 05api-3743202100% (1)
- Med, Legal, and Ethical IssuesDocument30 pagesMed, Legal, and Ethical IssuesJameston BostreNo ratings yet
- Chapter 09Document45 pagesChapter 09api-3743202100% (1)
- Chapter 12Document75 pagesChapter 12api-3743202No ratings yet
- Chapter 30Document72 pagesChapter 30api-3743202No ratings yet
- Chapter 10Document27 pagesChapter 10api-3743202No ratings yet
- Chapter 18Document84 pagesChapter 18api-3743202100% (2)
- NeuroemDocument51 pagesNeuroemJameston BostreNo ratings yet
- Chapter 15Document42 pagesChapter 15api-3743202No ratings yet
- Chapter 27Document47 pagesChapter 27api-3807629No ratings yet
- Chapter 16Document37 pagesChapter 16api-3743202No ratings yet
- Chapter 21Document33 pagesChapter 21api-3743202No ratings yet
- Chapter 24Document98 pagesChapter 24api-3807629No ratings yet
- Chapter 19Document32 pagesChapter 19api-3743202100% (1)
- Chapter 20Document52 pagesChapter 20api-3743202No ratings yet
- Chapter 29Document93 pagesChapter 29api-3743202No ratings yet
- Chapter 31Document52 pagesChapter 31api-3743202No ratings yet
- Chapter 28Document46 pagesChapter 28api-3743202No ratings yet
- HSC 4406 - Ch32Document68 pagesHSC 4406 - Ch32aeryll1305No ratings yet
- Chapter 33Document29 pagesChapter 33api-3743202No ratings yet
- Chapter 41Document26 pagesChapter 41api-3743202100% (2)
- Chapter 34Document28 pagesChapter 34api-3743202No ratings yet
- Chapter 37Document40 pagesChapter 37api-3743202No ratings yet
- Chapter 35Document48 pagesChapter 35api-3743202No ratings yet
- Chapter 36Document28 pagesChapter 36api-3743202No ratings yet
- Chapter 38Document43 pagesChapter 38api-3743202No ratings yet
- Health Assessment Long Answer QuestionsDocument11 pagesHealth Assessment Long Answer QuestionsSraddha Patel50% (2)
- Oxygenation NCM 103Document10 pagesOxygenation NCM 103Richmond LacadenNo ratings yet
- Shock With Jugular Venous Distention: Clinical Review ArticleDocument9 pagesShock With Jugular Venous Distention: Clinical Review ArticlenevmerkaNo ratings yet
- Resident Chest Pain ModuleDocument7 pagesResident Chest Pain ModuleFatima ShoukatNo ratings yet
- The Relationship of Chest X-Ray in COVID-19 Patients and Disease Severity in Arifin Achmad General Hospital RiauDocument8 pagesThe Relationship of Chest X-Ray in COVID-19 Patients and Disease Severity in Arifin Achmad General Hospital RiauHangga WingitNo ratings yet
- Paroxysmal Nocturnal DyspneaDocument5 pagesParoxysmal Nocturnal DyspneanunungNo ratings yet
- Fluid Management PubmedDocument8 pagesFluid Management PubmedResti DwiuNo ratings yet
- ANANTARA - RESPI (Titz) Selalu Cross Check YaDocument24 pagesANANTARA - RESPI (Titz) Selalu Cross Check YaPuteri Fadillah ZahraNo ratings yet
- Pulmonary EdemaDocument20 pagesPulmonary EdemaMohmmad Lateef GanieNo ratings yet
- O2 TherapyDocument23 pagesO2 TherapyRenea Joy ArruejoNo ratings yet
- Congestive Heart Failure: Mulualem W.MD Dmu, Department of Internal Medicine For Ho StudentsDocument27 pagesCongestive Heart Failure: Mulualem W.MD Dmu, Department of Internal Medicine For Ho Studentsmuluneh birhaneNo ratings yet
- NCM 109 Rle: Absence Seizures, Type 1 Diabetes MellitusDocument4 pagesNCM 109 Rle: Absence Seizures, Type 1 Diabetes MellitusDarren RobertoNo ratings yet
- Care of Clients With Problems in OxygenationDocument8 pagesCare of Clients With Problems in OxygenationRed StohlNo ratings yet
- Postoperative Care: Nursing ManagementDocument25 pagesPostoperative Care: Nursing ManagementHarjotBrarNo ratings yet
- DAVIS MedSurg Notes Nurse S Clinical Pocket Guide FA Davis 2007Document242 pagesDAVIS MedSurg Notes Nurse S Clinical Pocket Guide FA Davis 2007amaliea234100% (1)
- Fluid Electrolytes and Acid Base BalanceDocument108 pagesFluid Electrolytes and Acid Base BalancesayednourNo ratings yet
- Philippine General HospitalDocument5 pagesPhilippine General HospitalMamski AnnNo ratings yet
- Cor Pulmonale: Anjela BaidyaDocument31 pagesCor Pulmonale: Anjela BaidyaAnjela BaidyaNo ratings yet
- Lec 2Document12 pagesLec 2zerish0208No ratings yet
- Swyer James MacLeod SyndromeDocument12 pagesSwyer James MacLeod Syndromeflori.bNo ratings yet
- NCP - Ineffective Breathing PatternDocument4 pagesNCP - Ineffective Breathing PatternPRINCESS KOBAYASHINo ratings yet
- Anesthetic Assesment & PremedicationDocument82 pagesAnesthetic Assesment & PremedicationahmedNo ratings yet
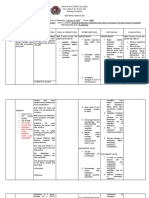
- C. Pathophysiology (Schematic Diagram) Predisposing Factors Precipitating FactorsDocument2 pagesC. Pathophysiology (Schematic Diagram) Predisposing Factors Precipitating FactorsMarynette MapaNo ratings yet
- Phosphorus: Nora Alnaqbi Huda Ibrahim AliaDocument15 pagesPhosphorus: Nora Alnaqbi Huda Ibrahim Aliacaramel109No ratings yet
- Review of SystemsDocument3 pagesReview of SystemsSusan BoyleNo ratings yet
- Focused Cardiac AssessmentDocument23 pagesFocused Cardiac AssessmentBonibel Bee Parker100% (2)
- First Responder NotesDocument8 pagesFirst Responder Notesjoe_a_salvatoreNo ratings yet