You might also like
- HW 7 Francis 3Document2 pagesHW 7 Francis 3api-240690004No ratings yet
- Great Starts Breakfast Survey ReportDocument42 pagesGreat Starts Breakfast Survey Reportapi-240690004No ratings yet
- Timelineupdated 1 15Document1 pageTimelineupdated 1 15api-240690004No ratings yet
- Yst - GSWB InforgraphicDocument2 pagesYst - GSWB Inforgraphicapi-240690004No ratings yet
- Di Resume 2 8Document2 pagesDi Resume 2 8api-240690004No ratings yet
- HW 7 Francis 2Document1 pageHW 7 Francis 2api-240690004No ratings yet
- 1 Fashionshowinvitation2013Document1 page1 Fashionshowinvitation2013api-240690004No ratings yet
- Infusionconfusion 6Document1 pageInfusionconfusion 6api-240690004No ratings yet
- 4 Proposal FinalDocument28 pages4 Proposal Finalapi-240690004No ratings yet
- 4 Progressive Growth EssayDocument2 pages4 Progressive Growth Essayapi-240690004No ratings yet
- 3 MethodsresearchproposalDocument11 pages3 Methodsresearchproposalapi-240690004No ratings yet
- 2 SBH Final PaperDocument12 pages2 SBH Final Paperapi-240690004No ratings yet
- 4 Bios Homework 2Document4 pages4 Bios Homework 2api-240690004No ratings yet
- Health-Education Plan For Richard BowmanDocument8 pagesHealth-Education Plan For Richard Bowmanapi-240690004No ratings yet
- 3 Casestudyfinal9 23afDocument12 pages3 Casestudyfinal9 23afapi-240690004No ratings yet
- 2 SBH BrochureoriginalDocument2 pages2 SBH Brochureoriginalapi-240690004No ratings yet
- 1 Briefing MemoDocument2 pages1 Briefing Memoapi-240690004No ratings yet
- 1 Fashionshowinvitation2013Document1 page1 Fashionshowinvitation2013api-240690004No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- KSKV Etn1013 - Electronic Schematic DrawingDocument12 pagesKSKV Etn1013 - Electronic Schematic DrawingNur Hafizah RazaliNo ratings yet
- Toward An Ecological Theory of Autism: January 2001Document31 pagesToward An Ecological Theory of Autism: January 2001carola1344No ratings yet
- Barrier Analysis PaperDocument8 pagesBarrier Analysis PaperGustavo DucaNo ratings yet
- Suicidepreventiondraft 2Document3 pagesSuicidepreventiondraft 2api-305982723No ratings yet
- Peet CurriculumvitaeDocument7 pagesPeet Curriculumvitaeapi-405364092No ratings yet
- FFM113: Fundamentals of Theatre and Film Production Management Lecturer: Raja Nor Aminah Binti Raja AyobDocument3 pagesFFM113: Fundamentals of Theatre and Film Production Management Lecturer: Raja Nor Aminah Binti Raja AyobAKMAL DANISH ALIPENo ratings yet
- The Militant Song Movement in Latin America Chile,... - (6 The Rhythm of Values Poetry and Music in Uruguay, 1960 1985)Document22 pagesThe Militant Song Movement in Latin America Chile,... - (6 The Rhythm of Values Poetry and Music in Uruguay, 1960 1985)Flavia ManciniNo ratings yet
- CI Project Proposal TemplateDocument6 pagesCI Project Proposal TemplateDarien Tayag Aloro100% (3)
- The ICF A Framework For Setting Goals For Children With Speech Impairment PDFDocument21 pagesThe ICF A Framework For Setting Goals For Children With Speech Impairment PDFRita GonçalvesNo ratings yet
- Nepf Teacher Professional Responsibilities Rubric With EvidDocument16 pagesNepf Teacher Professional Responsibilities Rubric With Evidapi-278277795No ratings yet
- Shouldice Hospital LTD: Group Case presentation-NMP25Document9 pagesShouldice Hospital LTD: Group Case presentation-NMP25Krishna TiwariNo ratings yet
- Power, Politics N EmpowermentDocument25 pagesPower, Politics N EmpowermentMade Candra SwadayaNo ratings yet
- Chanakya National Law UniversityDocument20 pagesChanakya National Law UniversityManini JaiswalNo ratings yet
- Vineyard Model - Prayer For HealingDocument6 pagesVineyard Model - Prayer For HealingNickNo ratings yet
- Assignment #1 Clinical PsychologyDocument17 pagesAssignment #1 Clinical PsychologyKaren NguyenNo ratings yet
- 4567 Main StreetDocument3 pages4567 Main StreetNajus NaaNo ratings yet
- Chapter 3-Managing Yourself To Get Things Done: True/FalseDocument12 pagesChapter 3-Managing Yourself To Get Things Done: True/FalsedavidNo ratings yet
- The Social BrainDocument41 pagesThe Social Brainchelseabaldo020890No ratings yet
- What Is ComprehensionDocument10 pagesWhat Is ComprehensionCm AgustinNo ratings yet
- Sentence Fragments: Use This Flowchart To Test For Sentence CompletenessDocument2 pagesSentence Fragments: Use This Flowchart To Test For Sentence CompletenessCathlyn LiNo ratings yet
- 2019 - An Mhealth Intervention For The Treatment of Patients With An Eating Disorder - A Multicenter Randomized Controlled TrialDocument13 pages2019 - An Mhealth Intervention For The Treatment of Patients With An Eating Disorder - A Multicenter Randomized Controlled TrialpabobadillaNo ratings yet
- Alphabet-Vocabulary-Flashcards - ListoDocument52 pagesAlphabet-Vocabulary-Flashcards - ListonanolakesNo ratings yet
- Be Set Free Fast (BSFF)Document8 pagesBe Set Free Fast (BSFF)Panther MelchizedekNo ratings yet
- Community PsychologyDocument5 pagesCommunity PsychologyKilliam WettlerNo ratings yet
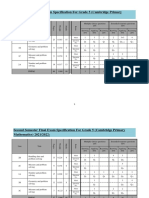
- Grade 5 Specifications CambridgeDocument2 pagesGrade 5 Specifications CambridgekatyaNo ratings yet
- Mory 2016Document35 pagesMory 2016daniela fonnegraNo ratings yet
- ESL Lesson PlanDocument4 pagesESL Lesson PlanRalph Julius DomingoNo ratings yet
- Digital Lesson PlanDocument5 pagesDigital Lesson Planapi-325767293No ratings yet
- Final ExamDocument5 pagesFinal Examkristenereeves100% (10)
- Visual Arts - Evic: This Are Lines Poised For ActionDocument6 pagesVisual Arts - Evic: This Are Lines Poised For Actionjohn evic aranteNo ratings yet