You might also like
- Handbook Emergency Cardiovascular Care Healthcare Providers PDFDocument2 pagesHandbook Emergency Cardiovascular Care Healthcare Providers PDFnoble78650% (4)
- Quiz ResultsDocument3 pagesQuiz Resultsasif charsiNo ratings yet
- ALS Manual PDFDocument74 pagesALS Manual PDFBlack Owell100% (1)
- Emergency DrugsDocument2 pagesEmergency DrugsCote ParejaNo ratings yet
- 2020 ECC GuidelinesDocument32 pages2020 ECC GuidelinesKevin Michael Reyes Roque100% (1)
- Ghiduriresuscitare2010V2 UnlockedDocument938 pagesGhiduriresuscitare2010V2 UnlockedMadalina Blaga100% (1)
- Basic Life Support (BLS) Provider HandbookFrom EverandBasic Life Support (BLS) Provider HandbookRating: 5 out of 5 stars5/5 (2)
- Advanced Clinical Therapies in Cardiovascular Chinese MedicineFrom EverandAdvanced Clinical Therapies in Cardiovascular Chinese MedicineNo ratings yet
- BLS Provider: Jeffree Perez, RNDocument2 pagesBLS Provider: Jeffree Perez, RNAbdussalam BacaramanNo ratings yet
- BLS Adult Cardiac Arrest Algorithm 2015 UpdateDocument2 pagesBLS Adult Cardiac Arrest Algorithm 2015 UpdateRS Harum Sisma MedikaNo ratings yet
- CARESCAPE R860 Modes of Ventilation FINAL Rev 3 JB72469XXDocument47 pagesCARESCAPE R860 Modes of Ventilation FINAL Rev 3 JB72469XXMichael Levit100% (1)
- Aha 2010 PDFDocument32 pagesAha 2010 PDFaldasimbolonNo ratings yet
- Resusgl 2010Document157 pagesResusgl 2010Salman IslamNo ratings yet
- AHA CPR Guidelines 2010Document2 pagesAHA CPR Guidelines 2010Alvin Roel NiervaNo ratings yet
- 2015 CPR and ECC Guidelines UpdateDocument50 pages2015 CPR and ECC Guidelines UpdateAmy KochNo ratings yet
- Resusitasi AnastesiDocument15 pagesResusitasi AnastesiFannia ReynathaNo ratings yet
- Adult Advanced Life SupportDocument14 pagesAdult Advanced Life SupportAnonymous TT7aEIjhuhNo ratings yet
- High Quality CPR Can Prevent ComplicationsDocument8 pagesHigh Quality CPR Can Prevent ComplicationsAnisa PutriNo ratings yet
- Advanced Life Support-RESSU CouncilDocument30 pagesAdvanced Life Support-RESSU CouncilGigel DumitruNo ratings yet
- Adult BLS Theoretical GuidelinesDocument31 pagesAdult BLS Theoretical GuidelinesclubsanatateNo ratings yet
- Basic Life Support - Provider Manual 2020Document87 pagesBasic Life Support - Provider Manual 2020Mohamad El Shar100% (1)
- CPR PDFDocument37 pagesCPR PDFArdhi AgustjikNo ratings yet
- Bls Healthcare ProvidersDocument36 pagesBls Healthcare ProvidersAshraf QutmoshNo ratings yet
- Clinical Guidelines Acute Rehab Management 2010 InteractiveDocument172 pagesClinical Guidelines Acute Rehab Management 2010 InteractivenathanaelandryNo ratings yet
- Tony Handley - New CPR Guidelines ExplainedDocument8 pagesTony Handley - New CPR Guidelines ExplainedJeaudeen JaleelNo ratings yet
- @literaturamedica BLS 2021Document94 pages@literaturamedica BLS 2021siracue22No ratings yet
- Guidelines For Adult Stroke Rehab and Recovery Ucm 485182Document117 pagesGuidelines For Adult Stroke Rehab and Recovery Ucm 485182Marcelo BenitezNo ratings yet
- Cardiac Rehab GuidelinesDocument265 pagesCardiac Rehab Guidelinesdorothy_put100% (1)
- 2010 CPR Guidelines: How The American Heart Association's CPR Guidelines Have Changed For 2010Document4 pages2010 CPR Guidelines: How The American Heart Association's CPR Guidelines Have Changed For 2010Raissa 'Icha' Nurwany RizalNo ratings yet
- Basic Life Supprt TrainingDocument16 pagesBasic Life Supprt TrainingFortune EyoNo ratings yet
- Irish Heart Foundation: Council For StrokeDocument117 pagesIrish Heart Foundation: Council For StrokeeimearNo ratings yet
- Cardiac RehabilitationDocument9 pagesCardiac Rehabilitationsara mohamedNo ratings yet
- Policy Statement2010Document23 pagesPolicy Statement2010unyilNo ratings yet
- BLS & AclsDocument13 pagesBLS & AclsadamNo ratings yet
- Concord CPR ManualDocument54 pagesConcord CPR ManualtntranNo ratings yet
- b4d1b448-94e9-43c0-a4d0-b9e526ba400dDocument68 pagesb4d1b448-94e9-43c0-a4d0-b9e526ba400dSayed ShandwielyNo ratings yet
- Highlights - ACLS - LinearizedDocument34 pagesHighlights - ACLS - LinearizedRayssaNo ratings yet
- Roles of Physiotherappist in ResuscitationDocument57 pagesRoles of Physiotherappist in Resuscitationabisinuola8No ratings yet
- From MedscapeCME Clinical BriefsDocument4 pagesFrom MedscapeCME Clinical Briefssraji64No ratings yet
- ATP-4 Update: Ronald E. Greer II M.DDocument15 pagesATP-4 Update: Ronald E. Greer II M.DReg GreerNo ratings yet
- Home Stroke VolDocument59 pagesHome Stroke VolElsy Pramitha SariNo ratings yet
- 2010 AHA Guidelines For CPR and ECC Summary TableDocument0 pages2010 AHA Guidelines For CPR and ECC Summary TableUtami HandayaniNo ratings yet
- Basic Life Support Perubahan Guideline AHA 2005-2010Document22 pagesBasic Life Support Perubahan Guideline AHA 2005-2010Momoh AlkaffNo ratings yet
- European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-Resuscitation CareDocument53 pagesEuropean Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-Resuscitation CareDaniel FajardoNo ratings yet
- Basic Life Support BLS Provider Manual A Comprehensive Guide Covering The Latest 2020 Guidelines 1st Edition M Mastenbjörk S Meloni Medical CreationsDocument54 pagesBasic Life Support BLS Provider Manual A Comprehensive Guide Covering The Latest 2020 Guidelines 1st Edition M Mastenbjörk S Meloni Medical Creationsmarie.akins223100% (4)
- Guidelines For CPR and ECC 2020Document29 pagesGuidelines For CPR and ECC 2020Pattih TibbitNo ratings yet
- Renu VHDDocument91 pagesRenu VHDRenu KhedekarNo ratings yet
- Cardiac RehabilitationDocument19 pagesCardiac RehabilitationAstrid Karina PutriNo ratings yet
- Top Ten Research Priorities Relating To Stroke Nursing - AshxDocument34 pagesTop Ten Research Priorities Relating To Stroke Nursing - Ashxahmadalipoland25No ratings yet
- Philippine Heart Association Council On Cardiopulmonary ResuscitationDocument4 pagesPhilippine Heart Association Council On Cardiopulmonary Resuscitationailyn pinedaNo ratings yet
- Part 3 - Adult Basic and Advanced Life Support - 2020 American Heart Association Guidelines For Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (001-050)Document50 pagesPart 3 - Adult Basic and Advanced Life Support - 2020 American Heart Association Guidelines For Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (001-050)odaliz.berrocalNo ratings yet
- Part 3 - Adult Basic and Advanced Life Support - 2020 American Heart Association Guidelines For Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (001-222)Document222 pagesPart 3 - Adult Basic and Advanced Life Support - 2020 American Heart Association Guidelines For Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (001-222)odaliz.berrocalNo ratings yet
- AHA/ASA Guideline: Guidelines For The Early Management of Patients With Acute Ischemic StrokeDocument64 pagesAHA/ASA Guideline: Guidelines For The Early Management of Patients With Acute Ischemic StrokefadilNo ratings yet
- Pediatric Cardiac Arrest AlgorithmDocument27 pagesPediatric Cardiac Arrest AlgorithmLinna AndrianiNo ratings yet
- Manipal Manual of Resuscitation - 4th EditionDocument73 pagesManipal Manual of Resuscitation - 4th EditionAshlita Mendonca100% (2)
- J. Am. Coll. Cardiol.: by On December 27, 2011 Downloaded FromDocument11 pagesJ. Am. Coll. Cardiol.: by On December 27, 2011 Downloaded FromAnonymous gpNr8cLWNo ratings yet
- Advanced Cardiac Life Support (ACLS) Provider HandbookFrom EverandAdvanced Cardiac Life Support (ACLS) Provider HandbookRating: 5 out of 5 stars5/5 (1)
- Total Knee Replacement and Rehabilitation: The Knee Owner's ManualFrom EverandTotal Knee Replacement and Rehabilitation: The Knee Owner's ManualRating: 5 out of 5 stars5/5 (6)
- Invoice Februari OtwDocument43 pagesInvoice Februari OtwAnnissa Puspa JNo ratings yet
- Airway Catalog MDT 2019 With Link Web 2Document5 pagesAirway Catalog MDT 2019 With Link Web 2Adhe TebetNo ratings yet
- Equipment List: Equipment and Supplies Quantity Needed Learning/Testing Station Equipment NeededDocument3 pagesEquipment List: Equipment and Supplies Quantity Needed Learning/Testing Station Equipment NeededVictoriano MendezNo ratings yet
- 12 02 2013 5010Document15 pages12 02 2013 5010apoorba_ganguly923No ratings yet
- Table 18-3 - Commonly Used Ventilator ModesDocument2 pagesTable 18-3 - Commonly Used Ventilator ModesDragutin PetrićNo ratings yet
- CPR & First AidDocument125 pagesCPR & First AidEvaNatashaNo ratings yet
- Nennyelyaniginting,+7 +Yoani+Maria+Vianney+Bita+AtyDocument10 pagesNennyelyaniginting,+7 +Yoani+Maria+Vianney+Bita+AtyBayu IsmoyoNo ratings yet
- Use of A New Videolaryngoscope (Glidescope®) in The Management of A Difficult AirwayDocument3 pagesUse of A New Videolaryngoscope (Glidescope®) in The Management of A Difficult AirwayAnonymous qqgN8jNo ratings yet
- Medtronic. Mcgrath Vdieo Laryngoscope. BrochureDocument4 pagesMedtronic. Mcgrath Vdieo Laryngoscope. Brochuremesssaoudi faresNo ratings yet
- Daftar Inventaris Trolley Emergency emDocument4 pagesDaftar Inventaris Trolley Emergency emYuli SukmawatiNo ratings yet
- Critical Care Nurses Association of The PhilippinesDocument2 pagesCritical Care Nurses Association of The Philippinesnurseharebee100% (2)
- Daftar Nama Obat Higt Alert 11-2022Document2 pagesDaftar Nama Obat Higt Alert 11-2022Mulyani NangNo ratings yet
- Ners. Nita Rosnida, S.Kep: Basic Life Support and Firts AidDocument2 pagesNers. Nita Rosnida, S.Kep: Basic Life Support and Firts AidMiki MarzukiNo ratings yet
- Basic Life Support Chart.: B-BreathingDocument1 pageBasic Life Support Chart.: B-BreathingOlga OrtegaNo ratings yet
- Pengantar SL CPRDocument19 pagesPengantar SL CPRHana SinurayaNo ratings yet
- CEDIVA Dénia, Training Center in Difficult Airway ManagementDocument29 pagesCEDIVA Dénia, Training Center in Difficult Airway ManagementCEDIVA DeniaNo ratings yet
- Modes of Ventilation H L en A02 01a NPDocument55 pagesModes of Ventilation H L en A02 01a NPSayan SenNo ratings yet
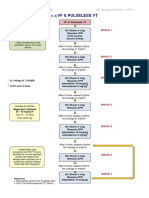
- VF & Pulseless VTDocument1 pageVF & Pulseless VTmadimadi11No ratings yet
- ACLS 2020 Update FOR CMEDocument51 pagesACLS 2020 Update FOR CMEyrx8k8j9qyNo ratings yet
- Circ Trial FlyerDocument1 pageCirc Trial FlyerForum PompieriiNo ratings yet
- Algo Pals BLS Pediatric Cardiac ArrestDocument1 pageAlgo Pals BLS Pediatric Cardiac ArrestSiti NabilaNo ratings yet
- 03MED1AGO2017Document292 pages03MED1AGO2017Elison CarvalhoNo ratings yet
- SYDocument54 pagesSYDimos MastroNo ratings yet
- Crash Cart Check ListDocument2 pagesCrash Cart Check ListMenGuitarNo ratings yet
- Intubasi - Dr. Hasan SpAnDocument42 pagesIntubasi - Dr. Hasan SpAnAlessia Wyneini TirzaNo ratings yet