You might also like
- Hoarding: Summary: Compulsive Hoarding (Aka Pathological Hoarding) Is Acquiring PossessionsDocument7 pagesHoarding: Summary: Compulsive Hoarding (Aka Pathological Hoarding) Is Acquiring Possessionsmazarica456No ratings yet
- The Noonday Demon: An Atlas of Depression by Andrew Solomon (Excerpt)Document28 pagesThe Noonday Demon: An Atlas of Depression by Andrew Solomon (Excerpt)Simon and Schuster63% (35)
- Pulmonary HTNDocument51 pagesPulmonary HTNMuhammad HaekalNo ratings yet
- Hypertension For StudentsDocument64 pagesHypertension For StudentsNajib Al FatinNo ratings yet
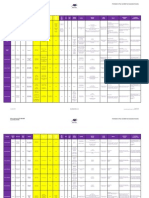
- QTC Flow Diagram With Medications Final Dec 17 A3 With LogosDocument1 pageQTC Flow Diagram With Medications Final Dec 17 A3 With LogosMelissa MurilloNo ratings yet
- Pulmonary Artery HypertensionDocument21 pagesPulmonary Artery HypertensionAzizi Abd RahmanNo ratings yet
- 15 Penyakit Ulkus Peptikum (Regimen Pengobatan H.pylory)Document738 pages15 Penyakit Ulkus Peptikum (Regimen Pengobatan H.pylory)Nhoer100% (1)
- "Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareDocument51 pages"Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareSohil ElfarNo ratings yet
- Vernier CaliperDocument2 pagesVernier CaliperMechtek LabNo ratings yet
- GrashaDocument9 pagesGrashaLisha LiuNo ratings yet
- A Case Study On Parkinsons DiseaseDocument42 pagesA Case Study On Parkinsons DiseaseMark Tristan AsuncionNo ratings yet
- Case Presentation On Op PoisoningDocument34 pagesCase Presentation On Op PoisoningSwerika KotteNo ratings yet
- SOP Example - VIP HandlingDocument4 pagesSOP Example - VIP HandlingΑντώνης ΤσίκοςNo ratings yet
- Irrigation ManagementDocument185 pagesIrrigation Managementaravind ragavanNo ratings yet
- Management VasculopatyDocument23 pagesManagement VasculopatyAgus SusantoNo ratings yet
- A Case Report of A Patient With Pulmonary Arterial Hypertension Transitioned From Inhaled Iloprost To SelexipagDocument4 pagesA Case Report of A Patient With Pulmonary Arterial Hypertension Transitioned From Inhaled Iloprost To SelexipagLava calolaNo ratings yet
- Pulmonary Hypertension: Dya Andryan MD Sumedang General HospitalDocument32 pagesPulmonary Hypertension: Dya Andryan MD Sumedang General HospitalDya AndryanNo ratings yet
- 5 - Esc Guidence 2015 Pulmonary HypertensionDocument85 pages5 - Esc Guidence 2015 Pulmonary Hypertensionpuskommedic 003No ratings yet
- Acute DyspneaDocument37 pagesAcute Dyspneaisnaira imamNo ratings yet
- Pulmonary HTN Topic DiscussionDocument2 pagesPulmonary HTN Topic Discussionapi-648401824No ratings yet
- Selexipag 1-29-2016 (Richard Wells)Document49 pagesSelexipag 1-29-2016 (Richard Wells)Aditya MadhavpeddiNo ratings yet
- J Jcin 2022 10 004Document3 pagesJ Jcin 2022 10 004Ivan BitunjacNo ratings yet
- Presentasi Hipertensi BPJS 20518Document109 pagesPresentasi Hipertensi BPJS 20518Dody TamaraNo ratings yet
- Plasma Renin Activity and Aldosterone Concentration Are Not Altered by The Novel Calcium Channel Antagonist, Azelnidipine, in Hypertensive PatientsDocument7 pagesPlasma Renin Activity and Aldosterone Concentration Are Not Altered by The Novel Calcium Channel Antagonist, Azelnidipine, in Hypertensive Patientsrgp1089No ratings yet
- Case Study ThrombocytopeniaDocument8 pagesCase Study ThrombocytopeniaAmina TariqNo ratings yet
- Astra End HipDocument47 pagesAstra End HipIlze KonrādeNo ratings yet
- Hipertensi UrgensiDocument26 pagesHipertensi UrgensidiegoNo ratings yet
- Benza 2013Document8 pagesBenza 2013FRANCISCO VILLEGAS LIROLANo ratings yet
- Pedoman CopdDocument42 pagesPedoman CopddaranhtgNo ratings yet
- PAH Presentation SlidesDocument64 pagesPAH Presentation SlidesStacie PenkovaNo ratings yet
- Drug Monograph ExampleDocument6 pagesDrug Monograph ExampleAaltiyaNo ratings yet
- Pulmonary Arterial Hypertension TopicDocument32 pagesPulmonary Arterial Hypertension Topicapi-668691030No ratings yet
- Effects of An Antithrombin Drug in Patients With Subacute Exacerbations of Binswanger DiseaseDocument4 pagesEffects of An Antithrombin Drug in Patients With Subacute Exacerbations of Binswanger DiseaseFortune FireNo ratings yet
- Pentosan Polysulfate SodiumDocument1 pagePentosan Polysulfate SodiumOdessa FileNo ratings yet
- Treatment Protocol For Hypertension: Criteria For Diagnosing High Blood PressureDocument3 pagesTreatment Protocol For Hypertension: Criteria For Diagnosing High Blood PressureHarshitha LokeshNo ratings yet
- Case - Parkinson's Disease - pptx-2Document16 pagesCase - Parkinson's Disease - pptx-2Suhas CLNo ratings yet
- Ventilator-Associated Pneumonia (VAP)Document2 pagesVentilator-Associated Pneumonia (VAP)Maximilian BezzeghNo ratings yet
- Pulmonary Hypertension (PH) Cor Pulmonale (CP) : Professor Miron BOGDAN UMF "Carol Davila" BucurestiDocument63 pagesPulmonary Hypertension (PH) Cor Pulmonale (CP) : Professor Miron BOGDAN UMF "Carol Davila" BucurestiIoana VasileNo ratings yet
- Anameia PPT by Sandeep - FullDocument32 pagesAnameia PPT by Sandeep - Fullsravanthi100% (1)
- Study of The Role of Plasma Nt-Probnp in The Diagnosis of Heart FailureDocument5 pagesStudy of The Role of Plasma Nt-Probnp in The Diagnosis of Heart FailureMinerva Medical Treatment Pvt LtdNo ratings yet
- Paytonctrujillo - Er Drugs Nursing PharmacologyDocument9 pagesPaytonctrujillo - Er Drugs Nursing PharmacologyTricia Kaye IblanNo ratings yet
- Cilnidipine Adverse Effect in Hypertensive Chronic Kidney Disease Patient With Pedal Edema A Case ReportDocument3 pagesCilnidipine Adverse Effect in Hypertensive Chronic Kidney Disease Patient With Pedal Edema A Case Reportvyshnavi machirajuNo ratings yet
- Effect of Beraprost On Pulmonary Hypertension DueDocument6 pagesEffect of Beraprost On Pulmonary Hypertension DueBabebos 95No ratings yet
- Pomr Dewi 190919Document6 pagesPomr Dewi 190919emjehNo ratings yet
- PahDocument38 pagesPahannisNo ratings yet
- Co - PeptinDocument5 pagesCo - PeptinBandya SahooNo ratings yet
- Heart Failure Novotel BJMDocument20 pagesHeart Failure Novotel BJMFiqhiyatun PerdaniNo ratings yet
- DepartmentDocument7 pagesDepartmentmubarek abdurohemanNo ratings yet
- Infective eDocument29 pagesInfective eFuad Aman AbjNo ratings yet
- Jurding Hipertensi PulmonalDocument33 pagesJurding Hipertensi PulmonalRyu KangNo ratings yet
- 12-04-2021 IGD ALO + CKD On HD + Ascites + CAPDocument4 pages12-04-2021 IGD ALO + CKD On HD + Ascites + CAPFirdha RositaNo ratings yet
- Why Hard To Control Blood Pressure ?: Atma GunawanDocument35 pagesWhy Hard To Control Blood Pressure ?: Atma GunawanLies Pramana SariNo ratings yet
- BiopharmDocument9 pagesBiopharmquina mjNo ratings yet
- Novelmedicaltherapiesfor Pulmonaryarterial Hypertension: Caroline O 'Connell,, Dermot S. O 'Callaghan,, Marc HumbertDocument14 pagesNovelmedicaltherapiesfor Pulmonaryarterial Hypertension: Caroline O 'Connell,, Dermot S. O 'Callaghan,, Marc HumbertVijay KumarNo ratings yet
- Case Presentation On TIA and IHDDocument14 pagesCase Presentation On TIA and IHDS SAI BALAJI IYERNo ratings yet
- Hamed Alabad BPHDocument47 pagesHamed Alabad BPHHamed AlabadNo ratings yet
- Macabali GS2Document4 pagesMacabali GS2Christian Edward MacabaliNo ratings yet
- Early Post-Operative Pulmonary Hypertension Management in The ICUDocument34 pagesEarly Post-Operative Pulmonary Hypertension Management in The ICUari wijayantiNo ratings yet
- Acute Hepatic PorphyriasDocument11 pagesAcute Hepatic Porphyriasqayyum consultantfpscNo ratings yet
- Nt-Probnp: The Gold Standard Biomarker in Heart FailureDocument3 pagesNt-Probnp: The Gold Standard Biomarker in Heart FailureRiuin23No ratings yet
- MainDocument11 pagesMainDhonz R AdiwaramanNo ratings yet
- ANAMEIA PPT BY SandeepDocument32 pagesANAMEIA PPT BY SandeepSandeep ChakravarthyNo ratings yet
- 1anesthesia For Day Care Surgery 123Document49 pages1anesthesia For Day Care Surgery 123Parvathy R NairNo ratings yet
- PolycythemiaDocument26 pagesPolycythemiaFuad Aman AbjNo ratings yet
- Pulmonary Arterial Hypertension: Diagnosis and Evidence-Based TreatmentFrom EverandPulmonary Arterial Hypertension: Diagnosis and Evidence-Based TreatmentRobyn BarstNo ratings yet
- Prescolite Panorama Outdoor Lighting Catalog P-1 1966Document20 pagesPrescolite Panorama Outdoor Lighting Catalog P-1 1966Alan MastersNo ratings yet
- Mendozasalgado, 2005Document9 pagesMendozasalgado, 2005natss mateoNo ratings yet
- Nutrition Situation in GujaratDocument13 pagesNutrition Situation in GujaratDrRameem BlochNo ratings yet
- OCHEM Practice FinalDocument24 pagesOCHEM Practice FinalNoleNo ratings yet
- Panasonic KX-TD500 - Function GuideDocument1,574 pagesPanasonic KX-TD500 - Function GuideJuan Rivera100% (1)
- Waterproofing Catalogue: Parchem Construction SuppliesDocument20 pagesWaterproofing Catalogue: Parchem Construction SuppliesJet ToledoNo ratings yet
- Comparison Between Diferent International Exams To Evaluate EnglishDocument3 pagesComparison Between Diferent International Exams To Evaluate EnglishMiguel Antonio Gutierrez CorreaNo ratings yet
- Diagnosis and Treatment of Mitochondrial MyopathiesDocument14 pagesDiagnosis and Treatment of Mitochondrial MyopathiesUname EpithetoNo ratings yet
- Lathe MetalDocument1 pageLathe MetalSanthosh KumarNo ratings yet
- 10-17-23 Midtown Membership Agreement One PageDocument1 page10-17-23 Midtown Membership Agreement One PagebodybyonderNo ratings yet
- 9990 Scheme of Work (For Examination From 2020)Document96 pages9990 Scheme of Work (For Examination From 2020)AyaNo ratings yet
- Literature Review of Livestock and Poultry ManureDocument6 pagesLiterature Review of Livestock and Poultry ManureafdtlfbfpNo ratings yet
- Granular Sub-Base: Salient Features 2.1 MethodologyDocument2 pagesGranular Sub-Base: Salient Features 2.1 Methodologyvijay kumarNo ratings yet
- ICEL 1006 2012 - Emergency Lighting Design GuideDocument32 pagesICEL 1006 2012 - Emergency Lighting Design GuideSenn OdrapmasdNo ratings yet
- D-REED004 Summative Assessment 1: Samuel Barrett-Wayne E. AlcosebaDocument4 pagesD-REED004 Summative Assessment 1: Samuel Barrett-Wayne E. AlcosebaSamuel Barrett-WayneNo ratings yet
- SampleDocument3 pagesSampleRaguramNo ratings yet
- Seeds and Seeds Class 5 Notes CBSE EVS Chapter 5 (PDF)Document6 pagesSeeds and Seeds Class 5 Notes CBSE EVS Chapter 5 (PDF)krishna GNo ratings yet
- GEN BIO Plant and Animal CellDocument3 pagesGEN BIO Plant and Animal CellAira HaruneNo ratings yet
- ALLEN Scholarship Admission Test (ASAT) : Syllabus & PatternDocument1 pageALLEN Scholarship Admission Test (ASAT) : Syllabus & PatternAnshu KumarNo ratings yet
- HUAWEI P10 Lite Quick Start Guide (WAS-LX1, 02, 21 Lans, Dual, NEU) PDFDocument188 pagesHUAWEI P10 Lite Quick Start Guide (WAS-LX1, 02, 21 Lans, Dual, NEU) PDFritastoicaNo ratings yet
- Finals TVL-12 2019-2020Document3 pagesFinals TVL-12 2019-2020Mark Emerson MarinNo ratings yet
- POCKET GUIDE GOLD 2024 Ver 1.0 - WMVDocument53 pagesPOCKET GUIDE GOLD 2024 Ver 1.0 - WMVLina MaxlinNo ratings yet
- Excel FormatDocument38 pagesExcel FormatSaad QureshiNo ratings yet
- Imo Modul BDocument2 pagesImo Modul BTa BonNo ratings yet