You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Rocky Manual PDFDocument211 pagesRocky Manual PDFRaghul Ravi88% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Method Statement For Laying of MCC Duct and Civil Works For MCC NetworkDocument26 pagesMethod Statement For Laying of MCC Duct and Civil Works For MCC NetworkVenkadesh PeriathambiNo ratings yet
- No Quarter - 13 PDFDocument100 pagesNo Quarter - 13 PDFGorka Diaz PernasNo ratings yet
- RISC-V C Extension Instruction SetDocument17 pagesRISC-V C Extension Instruction SetTetricx The firstNo ratings yet
- Actinorhizal - WikipediaDocument5 pagesActinorhizal - WikipediahqctNo ratings yet
- Criteria For Patient Transfer From Recovery AreaDocument2 pagesCriteria For Patient Transfer From Recovery AreaDr Jisha TuNo ratings yet
- Hologram Packaging 6th P of MarketingDocument4 pagesHologram Packaging 6th P of MarketingCHANDER SHEKHAR JEENANo ratings yet
- Study and Realization of An ArducopterDocument66 pagesStudy and Realization of An ArducopterMostafa MelianiNo ratings yet
- Diskashur DT QSG EN FR DE ES ITDocument24 pagesDiskashur DT QSG EN FR DE ES ITAlucardNo ratings yet
- Micrologic 2.2 / 2.3-AB: Ratings (A) in at 40°C 100 160 240 400Document1 pageMicrologic 2.2 / 2.3-AB: Ratings (A) in at 40°C 100 160 240 400Slobodan SavicNo ratings yet
- Summary G1 Newton's LawsDocument1 pageSummary G1 Newton's Laws『IntTouchz』No ratings yet
- Smart Bus RMCR7 WebDocument111 pagesSmart Bus RMCR7 WebEder Alonso Cardenas CepedaNo ratings yet
- Teks 12a Nuclear Radiation Lesson NotesDocument5 pagesTeks 12a Nuclear Radiation Lesson Notesapi-236826747No ratings yet
- Surface Roughness Conversion Chart Tables - Engineers EdgeDocument10 pagesSurface Roughness Conversion Chart Tables - Engineers Edgejames.anitNo ratings yet
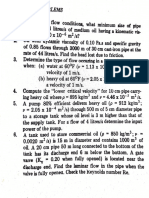
- Chapter 8 Exercise ProblemsDocument12 pagesChapter 8 Exercise ProblemsHalima Sibayan SawanganNo ratings yet
- Cost FM Sample PaperDocument6 pagesCost FM Sample PapercacmacsNo ratings yet
- 08 Chapter 3Document35 pages08 Chapter 3Jashanpreet SinghNo ratings yet
- Civil Engineering Sub-DisciplinesDocument4 pagesCivil Engineering Sub-DisciplinesRose Asto50% (2)
- Tabla de Capacidades. Grúa Manitowoc 30124CDocument16 pagesTabla de Capacidades. Grúa Manitowoc 30124CDavid RomoNo ratings yet
- Astm D5355 95Document1 pageAstm D5355 95gmpd.labNo ratings yet
- Grammar: Answer KeyDocument2 pagesGrammar: Answer KeyАааааа АааааааNo ratings yet
- The Limits of Thermal Comfort: Avoiding Overheating in European BuildingsDocument3 pagesThe Limits of Thermal Comfort: Avoiding Overheating in European BuildingsElissaNo ratings yet
- LO9&10Document13 pagesLO9&10Nine AranasNo ratings yet
- As 1289.5.8.1-2007 Methods of Testing Soils For Engineering Purposes Soil Comp Action and Density Tests - DeteDocument2 pagesAs 1289.5.8.1-2007 Methods of Testing Soils For Engineering Purposes Soil Comp Action and Density Tests - DeteSAI Global - APAC100% (1)
- Just Imagin Unit 2 Test 9th Grade 1-4 Final UPDATEDDocument4 pagesJust Imagin Unit 2 Test 9th Grade 1-4 Final UPDATEDalikhalilaseelNo ratings yet
- A Study On Chemical Grouting of Quartz Sand Binfeng ThesisDocument193 pagesA Study On Chemical Grouting of Quartz Sand Binfeng ThesisSafwat El RoubyNo ratings yet
- Runge-Kutta Methods - Wikipedia, The Free EncyclopediaDocument8 pagesRunge-Kutta Methods - Wikipedia, The Free EncyclopediaRadzi RasihNo ratings yet
- Harvesting and Marketing Vegetables: HELE 5: Quarter 2-W3-W4Document4 pagesHarvesting and Marketing Vegetables: HELE 5: Quarter 2-W3-W4Rajon G. TulioNo ratings yet
- Best VAGCOM Codes To Enable On Polo 6R - Page 4 - UK-POLOS - NET - THE VW Polo ForumDocument4 pagesBest VAGCOM Codes To Enable On Polo 6R - Page 4 - UK-POLOS - NET - THE VW Polo Forumvajihet327No ratings yet
- PASSION (Official) : Sponsored ContentDocument6 pagesPASSION (Official) : Sponsored ContentcodNo ratings yet